Neurobiology of Human Behavior & How Experience Modifies the Brain
Parietal-temporal-occipital association area
Area 5 and 7 are referred to as the Posterior Parietal Cortex (PPC). The parietal lobes are located between visual and somatosensory areas and receives input from both; they integrate visual and somatosensory information. Their main projection targets are premotor and motor cortical areas; therefore, lesions/damage of parietal cortices has profound effects on voluntary movements.
Function (deduced from recording discharges of neurons in trained monkeys)
Area 5
- Proper use of somatosensory information.
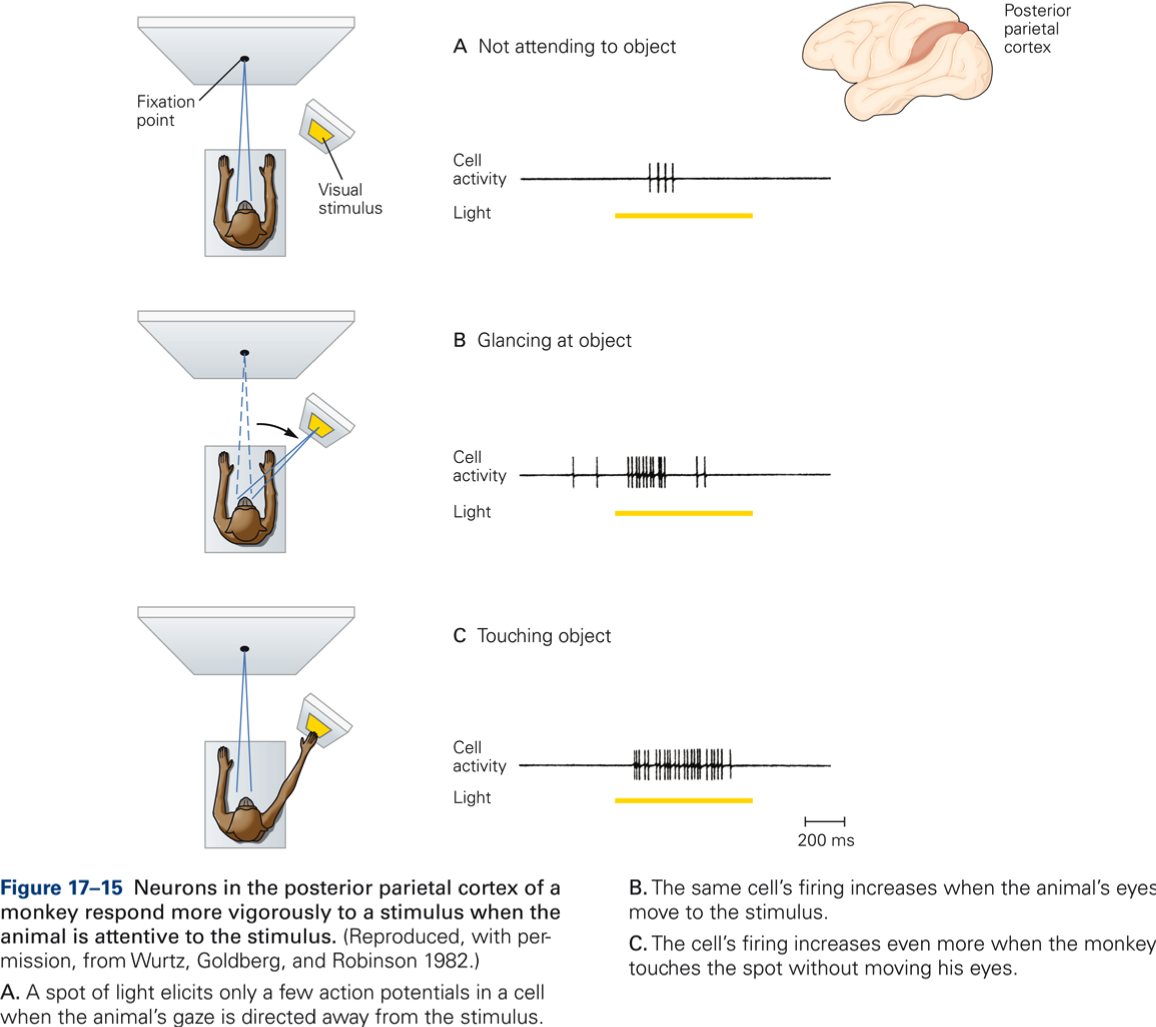
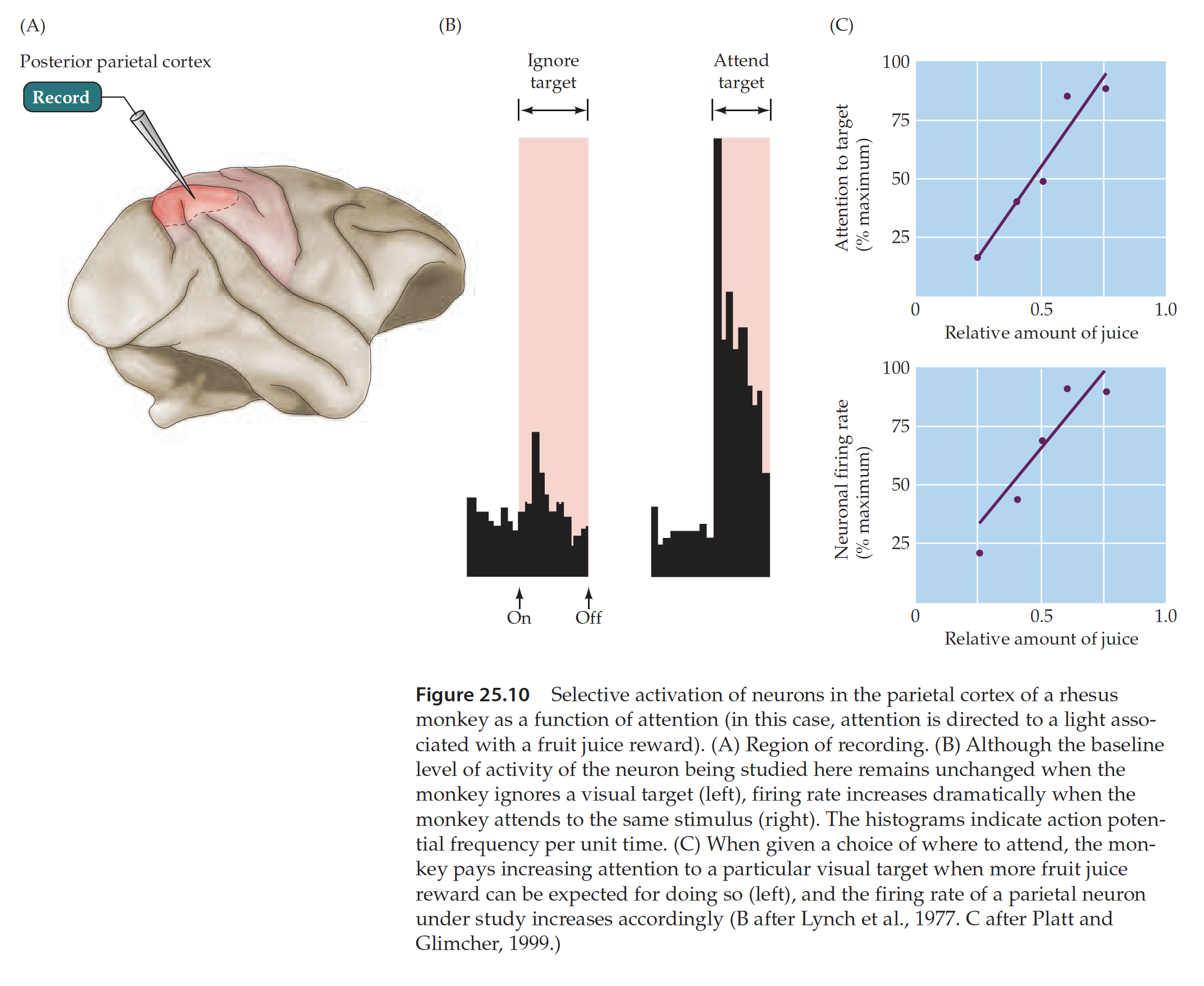
- Goal directed voluntary movements (increased discharge if stimulus relevant to behavior and attention is directed towards stimulus, e.g. reaching towards object of interest).
- Manipulation of objects (hand manipulation neurons, e.g. explorative touch).
Area 7
- Integration of visual and somatosensory information, e.g. visual guidance of movement.
In this video excerpt from NOVA scienceNOW: “How Does the Brain Work?” scientists team up with magician Apollo Robbins to research how our brains decide what to pay attention to. Test subjects are asked to watch a video of Apollo making a coin disappear while their eye position is measured 500 or 1,000 times a second. Neuroscientists learn that when people are visually tracking movement (like a magician moving a coin) there is more than one type of brain cell involved—one tracks motion and the other suppresses the background scene. [Source: PBS NOVA scienceNOW]
References
Macknik, Stephen L. and Susana Martinez-Conde with Sandra Blakeslee (2010). Sleights of Mind: What the Neuroscience of Magic Reveals About Our Everyday Deceptions, New York: Henry Holt and Co. [www.sleightsofmind.com].
Lesions in humans
Right and left hemispheres are not equivalent in function: left hemisphere is dominant for language and mental functions; the right is dominant for spatial relations and emotions. Therefore, lesions of association area of left side produce different set of symptoms than lesions right.
In general, lesions produce deficits in the transformation of sensory stimuli to adequate actions:
Agnosias
Impairment in understanding the interpretation (meaning) of stimulus, but not sensory experience as such, i.e. inability to perceive objects through otherwise normally functioning sensory channels.
- Astereognosia: inability to recognize the form of objects by touch, even though there is no pronounced loss of somatosensory sensitivity.
- Visual agnosia: a condition that can prevent people from recognizing objects and faces—including their own reflection.
Apraxias
Impaired ability to use tools
Impaired visual guidance of movements
Bilateral lesions: Balint syndrome
- Inability of voluntary eye movements (cannot direct gaze).
- Deficits in using visual guidance to grasp objects (optic ataxia). No paralysis, no visual deficits, but inability to estimate distances, sizes.
- Difficulty in attending to visual stimuli (patients only attend to one detail at a time).
Left side lesions: Gerstmann syndrome
- Finger agnosia: pt cannot distinguish fingers
- Agraphia: inability to write
- Alexia: inability to read
- Right/left confusion
- Dyscalculia: inability to do simple calculations
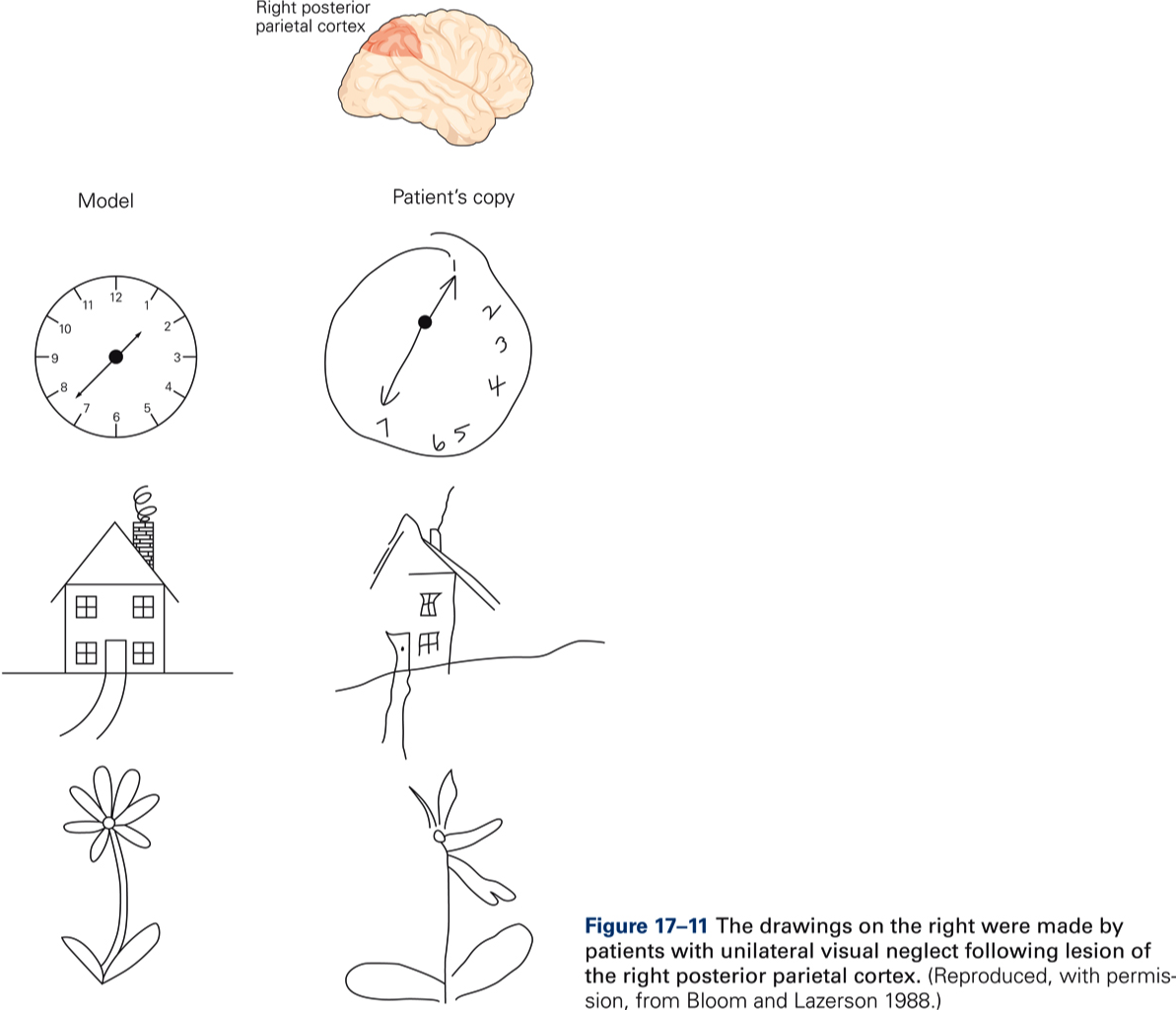
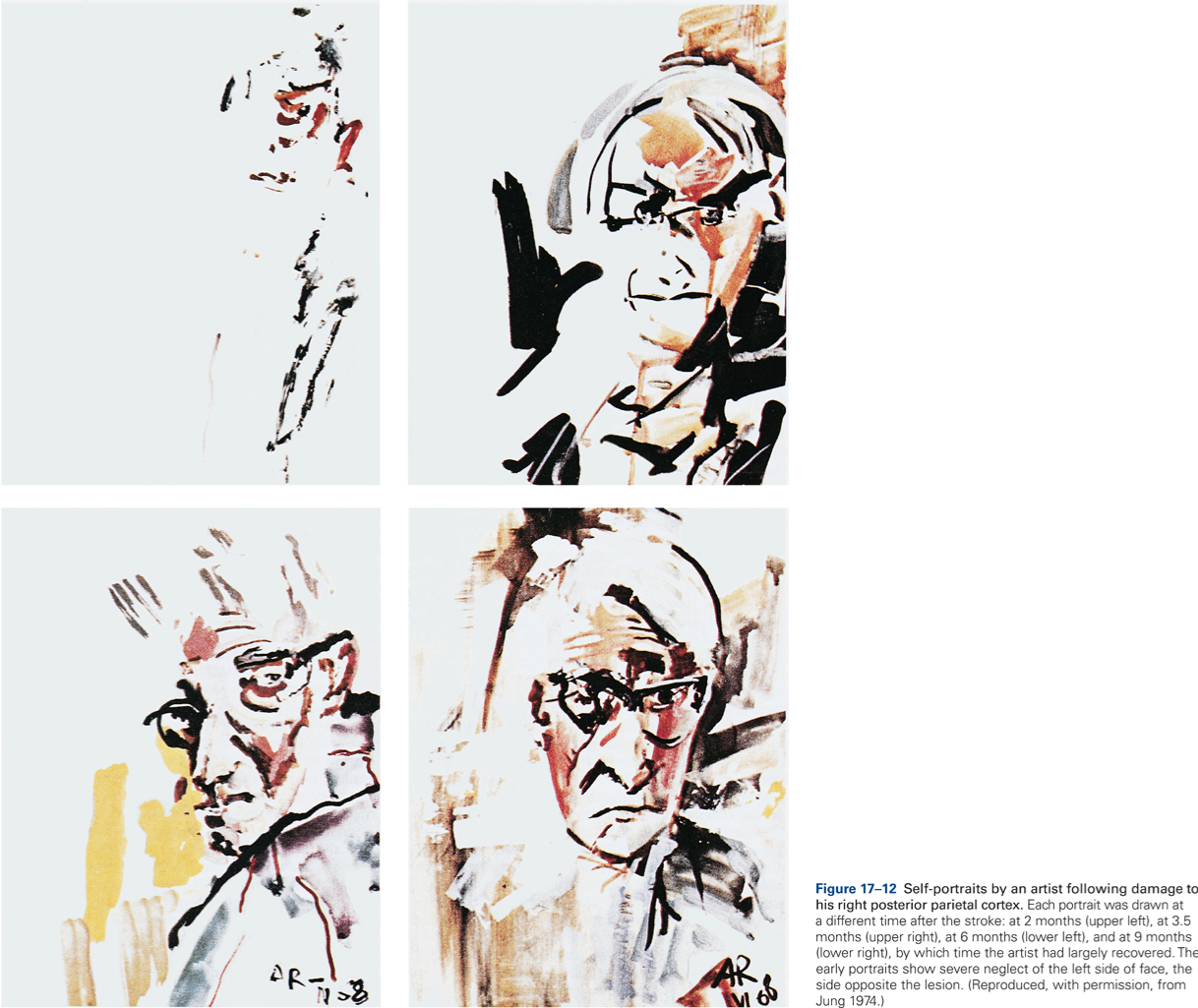
Right side lesions: Neglect syndrome, patients neglect contralateral body half and visual space.