Module 11: Vertebral Column, Thoracic Cage, and Trunk Wall
Learning Objectives:
By the end of this module, students will be able to:
-
Describe the components of the vertebral column and its regional variations.
- List the bones of the thoracic cavity and their key landmarks.
- Identify and describe the structure and function of the muscles of the thoracic and abdominal walls.
- Identify the neurovascular structures supplying and innervating the abdominal wall.
Terms to Know
|
Vertebral Column
|
Bones of the Thoracic Cage
Neurovascular Structures
Muscles of the Abdominal Wall
Muscles of the back
|
The vertebral column is also known as the spinal column or spine. It consists of a sequence of vertebrae (singular = vertebra), each of which is separated and united by an intervertebral disc. Together, the vertebrae and intervertebral discs form the vertebral column. It is a flexible column that supports the head, neck, and body and allows for their movements. It also protects the spinal cord, which passes down the back through openings in the vertebrae.
Regions of the Vertebral Column
*This content is covered in the pre-lecture assignment and will not be covered again in lecture.
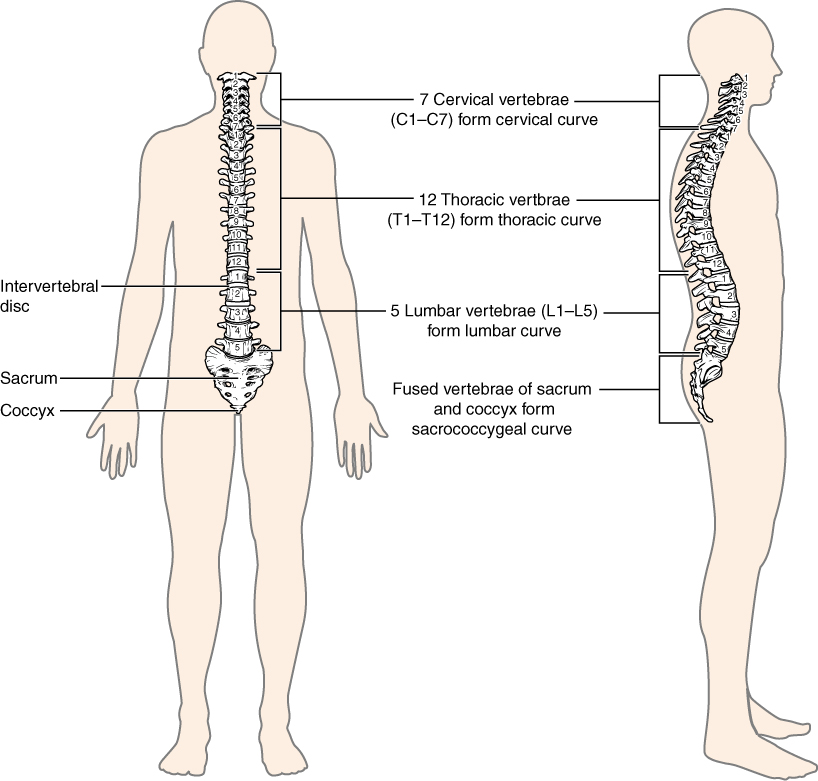
The vertebral column is subdivided into five regions, with the vertebrae in each area named for that region and numbered in descending order. There are seven cervical vertebrae in the neck, each designated with the letter “C” followed by its number. Superiorly, the C1 vertebra articulates (forms a joint) with the occipital condyles of the skull. Inferiorly, C1 articulates with the C2 vertebra, and so on. Below the cervical vertebrae are the 12 thoracic vertebrae, designated T1–T12. The lower back contains the L1–L5 lumbar vertebrae. The single sacrum, which is also part of the pelvis, is formed by the fusion of five sacral vertebrae. Similarly, the coccyx, or tailbone, results from the fusion of three to four small coccygeal vertebrae. However, the sacral and coccygeal fusions do not start until age 20 and are not completed until middle age.
Fun Fact – Cervical Vertebrae (-> you will not be assessed on this content)
An interesting anatomical fact is that almost all mammals have seven cervical vertebrae, regardless of body size. This means that there are large variations in the size of cervical vertebrae, ranging from the tiny cervical vertebrae of a shrew to the greatly elongated vertebrae in the neck of a giraffe. In a full-grown giraffe, each cervical vertebra is 11 inches tall.
Curvatures of the Vertebral Column
*This content is covered in the pre-lecture assignment and will be elaborated on in lecture.
The adult vertebral column does not form a straight line but instead has four curvatures along its length. These curves increase the vertebral column’s strength, flexibility, and ability to absorb shock. When the load on the spine is increased, by carrying a heavy backpack, the curvatures increase in depth (become more curved) to accommodate the extra weight. They then spring back when the weight is removed. The four adult curvatures are classified as either primary or secondary curvatures. Primary curves are retained from the original fetal curvature, while secondary curvatures develop after birth.
During fetal development, the body is flexed anteriorly into the fetal position, giving the entire vertebral column a single curvature that is concave anteriorly. In the adult, this fetal curvature is retained in two vertebral column regions as the thoracic curve, which involves the thoracic vertebrae, and the sacrococcygeal curve, formed by the sacrum and coccyx. Thus, each of these is called a primary curve because they are retained from the original fetal curvature of the vertebral column.
A secondary curve develops gradually after birth as the child learns to sit upright, stand, and walk. Secondary curves are concave posteriorly, opposite in direction to the original fetal curvature. The neck region’s cervical curve develops as the infant begins to hold their head upright when sitting. Later, as the child begins to stand and then to walk, the lumbar curve of the lower back develops.
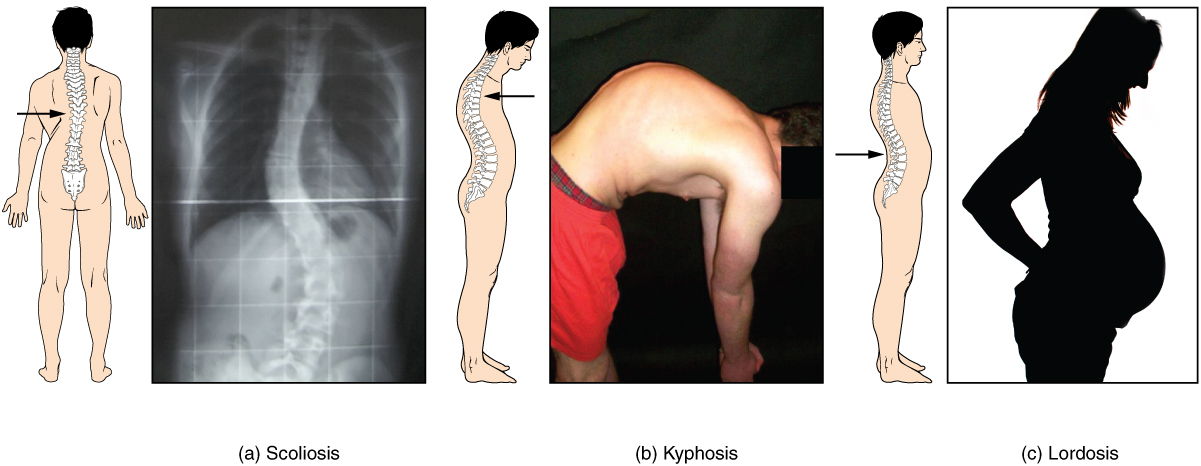
Disorders associated with the curvature of the spine include kyphosis (excessive posterior curvature of the thoracic region), lordosis (excessive anterior curvature of the lumbar region), and scoliosis (an abnormal, lateral curvature, accompanied by twisting of the vertebral column). Excessive vertebral curves can be identified while an individual stands in the anatomical position. Observe the vertebral profile from the side and then from behind to check for kyphosis or lordosis. Then have the person bend forward. If scoliosis is present, an individual will have difficulty bending directly forward, and the right and left sides of the back will not be level with each other in the bent position.
General Structure of a Vertebra
*This content is covered in the pre-lecture assignment and will not be covered again in lecture.
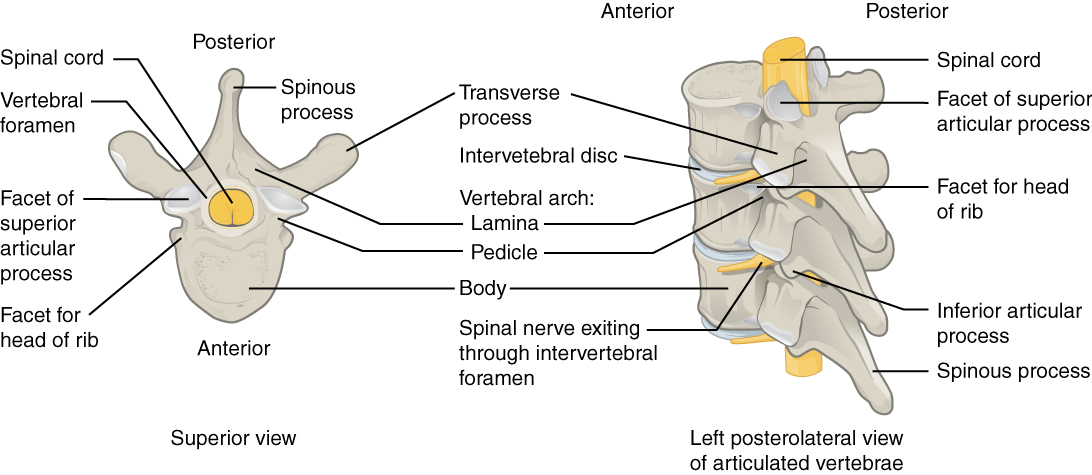
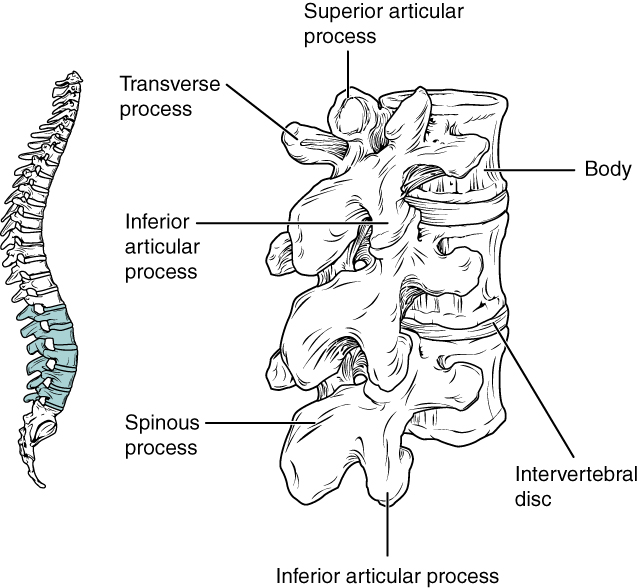
Within the vertebral column’s different regions, vertebrae vary in size and shape, but they all follow a similar structural pattern. A typical vertebra will consist of a body, a vertebral arch, and seven processes.
The body is the anterior portion of each vertebra and is the part that supports the body weight. Because of this, the vertebral bodies progressively increase in size and thickness going down the vertebral column. The bodies of adjacent vertebrae are separated and strongly united by an intervertebral disc.
The vertebral arch forms the posterior portion of each vertebra. It consists of four parts, the right and left pedicles and the right and left laminae. Each pedicle forms one of the lateral sides of the vertebral arch. The pedicles are anchored to the posterior side of the vertebral body. Each lamina forms part of the posterior roof of the vertebral arch. The large opening between the vertebral arch and body is the vertebral foramen, which contains the spinal cord. In the intact vertebral column, the vertebral foramina of all of the vertebrae align to form the vertebral (spinal) canal, which serves as the bony protection and passageway for the spinal cord down the back. When the vertebrae are aligned together in the vertebral column, notches in the margins of the pedicles of adjacent vertebrae together form an intervertebral foramen, the opening through which a spinal nerve exits from the vertebral column.
Seven processes arise from the vertebral arch. Each paired transverse process projects laterally and arises from the junction point between the pedicle and lamina. The single spinous process (vertebral spine) projects posteriorly at the midline of the back. The vertebral spines can easily be felt as a series of bumps just under the skin down the middle of the back. The transverse and spinous processes serve as important muscle attachment sites. A superior articular process extends or faces upward, and an inferior articular process faces or projects downward on each side of a vertebra. The paired superior articular processes of one vertebra join with the corresponding paired inferior articular processes from the next higher vertebra. These junctions form slightly moveable joints between the adjacent vertebrae. The shape and orientation of the articular processes vary in different vertebral column regions and play a major role in determining the type and range of motion available in each region.
Regional Modifications of Vertebrae
*This content is covered in the pre-lecture assignment and will not be covered again in lecture with the exception of C1, C2 and rib articulation.
In addition to the typical vertebra’s general characteristics described above, vertebrae also display characteristic size and structural features that vary between the different vertebral column regions. Thus, cervical vertebrae are smaller than lumbar vertebrae due to differences in the proportion of body weight that each supports. Thoracic vertebrae have sites for rib attachment, and the vertebrae that give rise to the sacrum and coccyx have fused into single bones.
Cervical Vertebrae
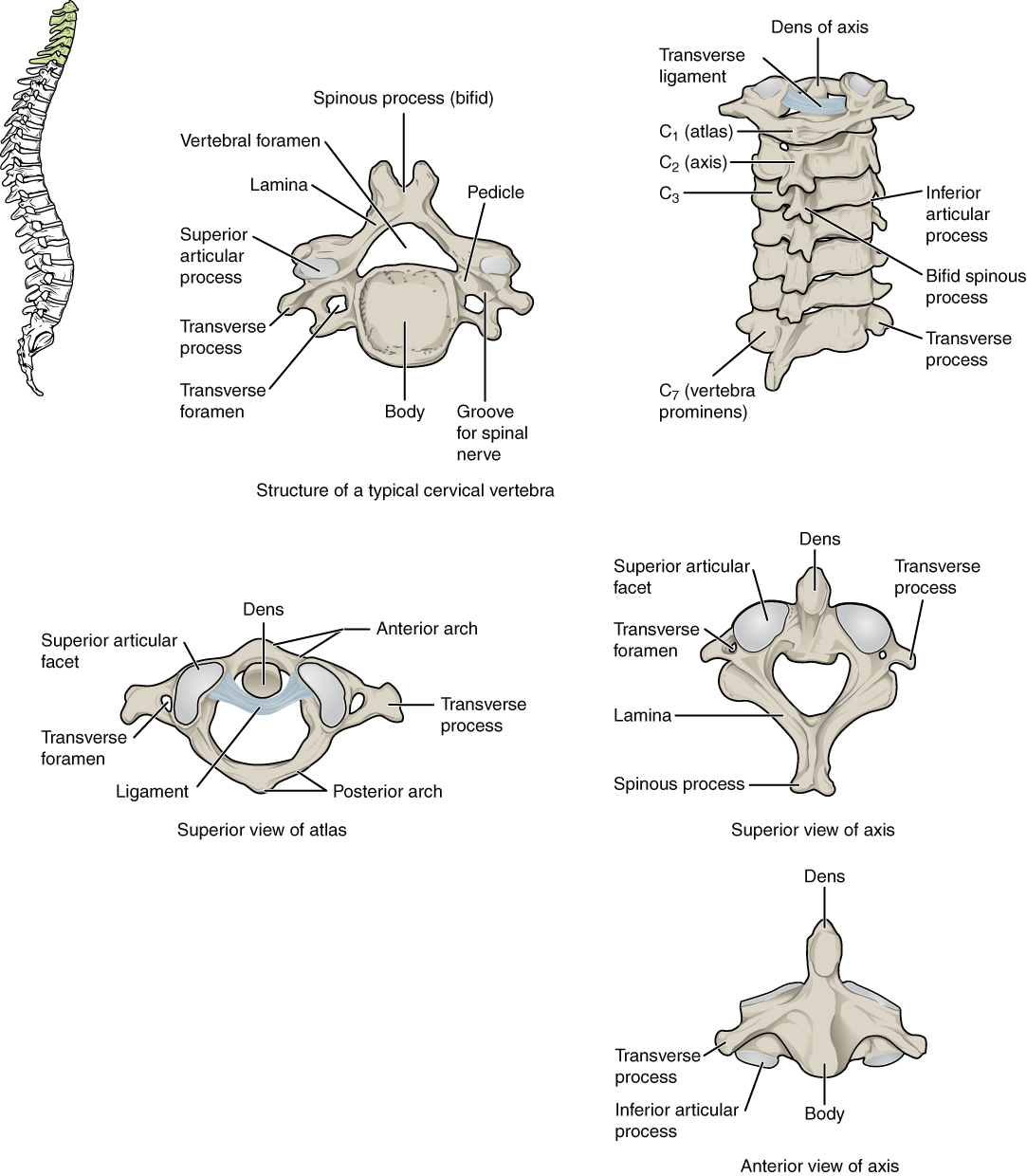
Typical cervical vertebrae, such as C4 or C5, have several characteristic features that differentiate them from thoracic or lumbar vertebrae. Cervical vertebrae have a small body, reflecting that they carry the least amount of body weight. Cervical vertebrae usually have a bifid (Y-shaped) spinous process. The C3–C6 vertebrae’s spinous processes are short, but the spine of C7 is much longer. You can find these vertebrae by running your finger down the midline of the posterior neck until you encounter the prominent C7 spine located at the base of the neck. The transverse processes of the cervical vertebrae are sharply curved (U-shaped) to allow for the cervical spinal nerves’ passage. Each transverse process also has an opening called the transverse foramen. An important artery that supplies the brain ascends the neck by passing through these openings. The superior and inferior articular processes of the cervical vertebrae are flattened and largely face upward or downward, respectively.
C1 and C2
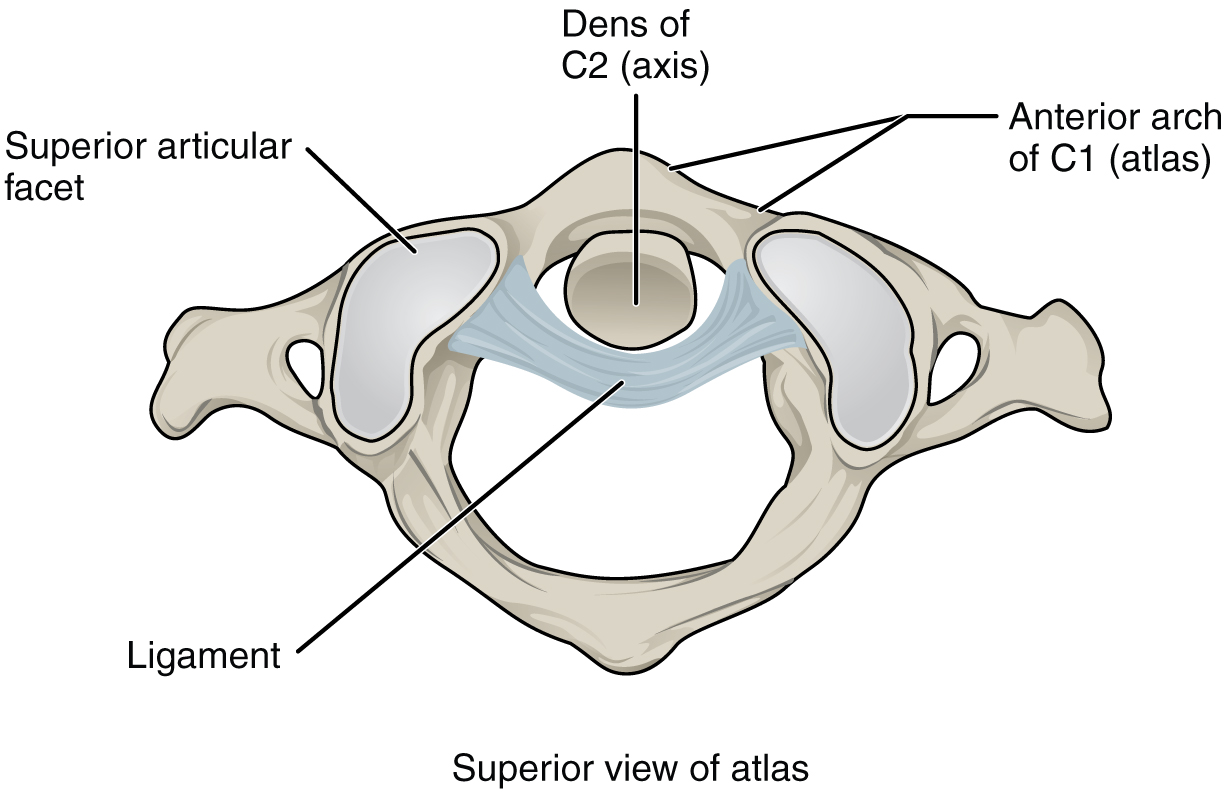
The first and second cervical vertebrae are further modified, giving each a distinctive appearance. The first cervical (C1) vertebra is also called the atlas because this vertebra supports the skull on top of the vertebral column (in Greek mythology, Atlas was the god who supported the heavens on his shoulders). The C1 vertebra does not have a body or spinous process. Instead, it is ring-shaped, consisting of an anterior arch and a posterior arch. The atlas’ transverse processes are longer and extend more laterally than do the transverse processes of any other cervical vertebrae. The superior articular processes face upward and are deeply curved for articulation with the occipital condyles on the base of the skull. The inferior articular processes are flat and face downward to join with the superior articular processes of the C2 vertebra.
The second cervical (C2) vertebra is called the axis because it serves as the axis for rotation when turning the head toward the right or left. In most respects, the axis resembles typical cervical vertebrae but is easily distinguished by the dens, a bony projection that extends upward from the vertebral body. The dens joins with the inner aspect of the anterior arch of the atlas, where it is held in place by the transverse ligament.
Thoracic Vertebrae
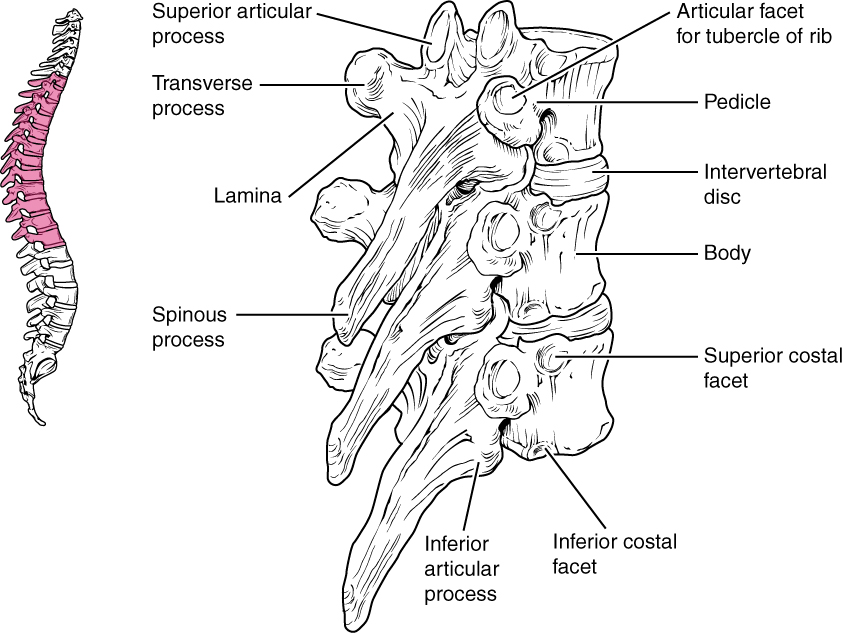
The bodies of the thoracic vertebrae are larger than those of cervical vertebrae. The characteristic feature for a typical midthoracic vertebra is the spinous process, which is long and has a pronounced downward angle that causes it to overlap the next inferior vertebra. The superior articular facets of thoracic vertebrae face posteriorly, and the inferior articular facets face anteriorly. These orientations are important determinants for the type and range of movements available to the thoracic region of the vertebral column.
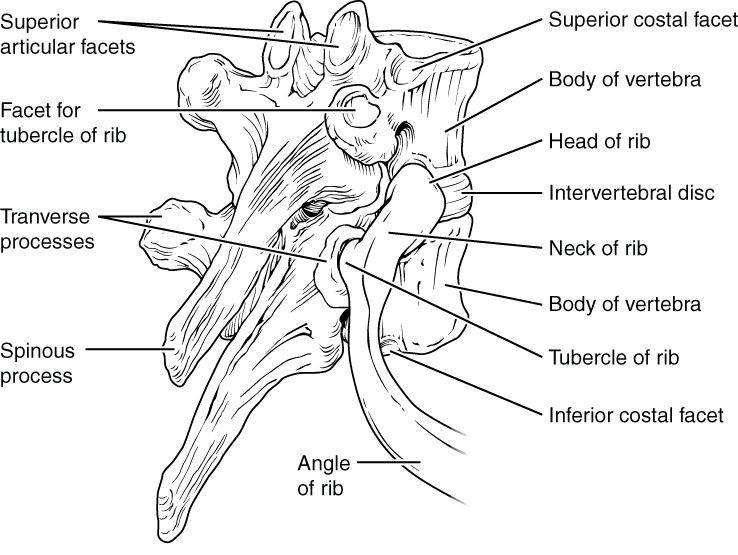
Thoracic vertebrae have several additional articulation sites, each of which is called a facet, where a rib is attached. Most thoracic vertebrae have two facets located on the lateral sides of the body, each of which is called a costal (demi)facet. These are for articulation with the head (end) of a rib. An additional facet is located on the transverse process for articulation with the tubercle of a rib.
Fun Facts – Facets and demifacets (-> you will not be assessed on this content)
A facet is a joint where either two vertebrae articulate, or where a rib articulates with a vertebra (sometimes called a costal facet). A costal facet is the site of attachment of a rib to the body or transverse process of a thoracic vertebra. A superior or inferior articular facet is where vertebrae above or below articulate with the next vertebrae at the superior or inferior articular process, respectively. In the context of this course, we often consider facets primarily as the articulation of a rib with a vertebra.
- T1 has a complete facet and an inferior demifacet – the body of T1 articulates with the head of Rib 1 and the inferior demifacet articulates with the head of Rib 2.
- T10-T12 have complete facets – the bodies of T10-T12 articulate with the heads of Ribs 10-12, respectively.
- T2-T9 all have demifacets.
- A demifacet is the articulation of the rib with the body of two different vertebrae (watch the video in the lecture module to see this articulation).
Lumbar Vertebrae
Lumbar vertebrae carry the greatest amount of body weight and are thus characterized by the vertebral body’s large size and thickness. They have short transverse processes and a short, blunt spinous process that projects posteriorly. The articular processes are large, with the superior process facing backward and the inferior facing forward.
Sacrum and Coccyx
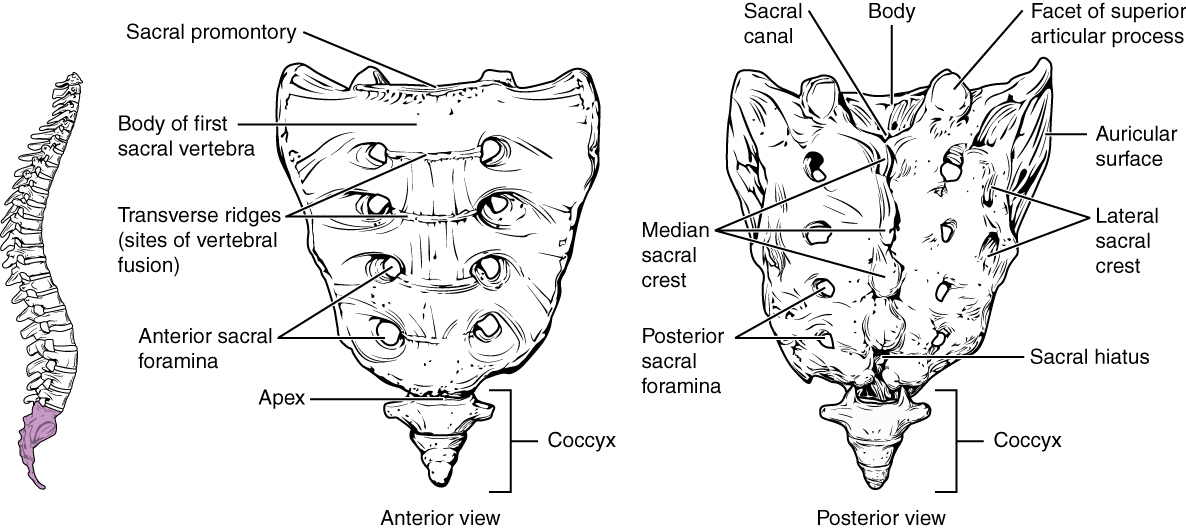
The sacrum is a triangular-shaped bone that is thick and wide across its superior base, where it is weight-bearing and then tapers down to an inferior, non-weight bearing apex. It is formed by the fusion of five sacral vertebrae, which does not begin until after the age of 20. On the anterior surface of the older adult sacrum, the lines of vertebral fusion can be seen as four transverse ridges. On the posterior surface, running down the midline, is the median sacral crest, a bumpy ridge that is the remnant of the fused spinous processes (median = “midline”; while medial = “toward, but not necessarily at, the midline”). Similarly, the fused transverse processes of the sacral vertebrae form the lateral sacral crest.
The sacral promontory is the anterior lip of the superior base of the sacrum. Lateral to this is the roughened auricular surface, which joins with the ilium portion of the hipbone to form the immobile sacroiliac joints of the pelvis. Passing inferiorly through the sacrum is a bony tunnel called the sacral canal, which terminates at the sacral hiatus near the sacrum’s inferior tip. The sacrum’s anterior and posterior surfaces have a series of paired openings called sacral foramina (singular = foramen) that connect to the sacral canal. Each of these openings is called a posterior (dorsal) sacral foramen or anterior (ventral) sacral foramen. These openings allow for the anterior and posterior branches of the sacral spinal nerves to exit the sacrum. The superior articular process of the sacrum, one of which is found on either side of the superior opening of the sacral canal, articulates with the inferior articular processes from the L5 vertebra.
The coccyx, or tailbone, is derived from the fusion of four very small coccygeal vertebrae. It articulates with the inferior tip of the sacrum. It is not weight-bearing in the standing position but may receive some bodyweight when sitting.
Intervertebral Discs and Ligaments of the Vertebral Column
*This content is covered in the pre-lecture assignment and will be elaborated on in lecture.
The bodies of adjacent vertebrae are strongly anchored to each other by an intervertebral disc. This structure provides padding between the bones during weight-bearing, and because it can change shape, it also allows for movement between the vertebrae. Although the total amount of movement available between any two adjacent vertebrae is small, when these movements are summed together along the vertebral column’s entire length, large body movements can be produced. Ligaments that extend along the length of the vertebral column also contribute to its overall support and stability.
Intervertebral Disc
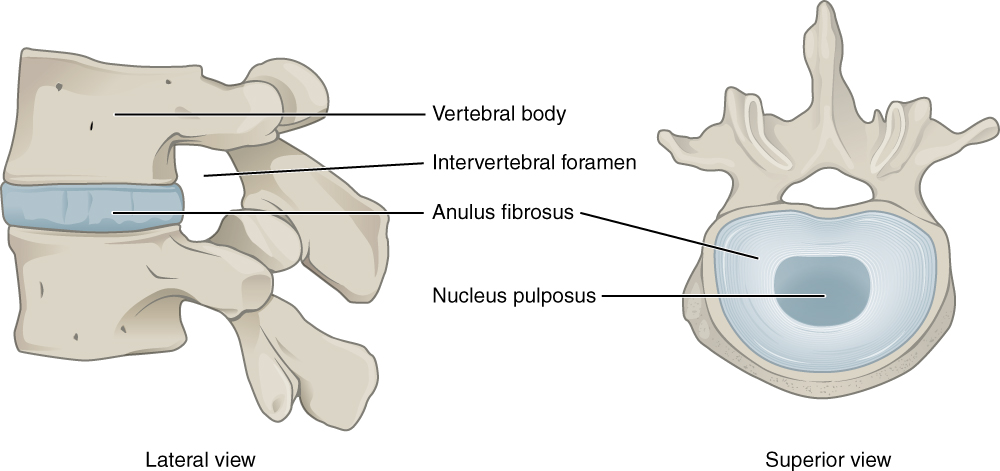
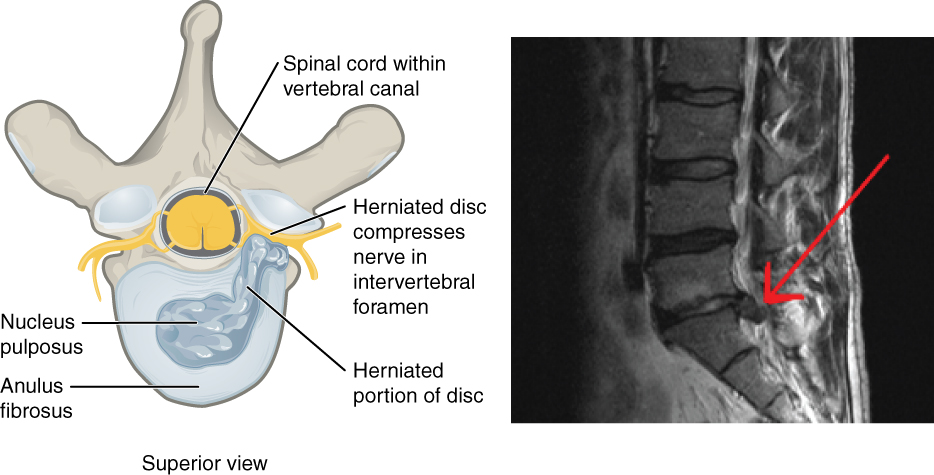
An intervertebral disc is a fibrocartilaginous pad that fills the gap between adjacent vertebral bodies. Each disc is anchored to the bodies of its adjacent vertebrae, thus strongly uniting these. The discs also provide padding between vertebrae during weight-bearing. Thus, intervertebral discs are thin in the cervical region and thickest in the lumbar region, which carries the most bodyweight. In total, the intervertebral discs account for approximately 25 percent of your body height between the top of the pelvis and the base of the skull. Intervertebral discs are also flexible and can change shape to allow for movements of the vertebral column.
Each intervertebral disc consists of two parts. The annulus fibrosus is the tough, fibrous outer layer of the disc. It forms a circle (annulus = “ring” or “circle”) and is firmly anchored to the outer margins of the adjacent vertebral bodies. Inside is the nucleus pulposus, consisting of a softer, more gel-like material. It has a high water content that serves to resist compression and thus is important for weight-bearing. With increasing age, the water content of the nucleus pulposus gradually declines. This causes the disc to become thinner, decreasing total body height somewhat, and reduces the disc’s flexibility and range of motion, making bending more difficult.
The gel-like nature of the nucleus pulposus also allows the intervertebral disc to change shape as one vertebra rocks side to side or forward and back in relation to its neighbors during movements of the vertebral column. Thus, bending forward causes compression of the disc’s anterior portion but an expansion of the posterior disc. If the posterior annulus fibrosus is weakened due to injury or increasing age, the pressure exerted on the disc when bending forward and lifting a heavy object can cause the nucleus pulposus to protrude posteriorly through the annulus fibrosus, resulting in a herniated disc (“ruptured” or “slipped” disc). The posterior bulging of the nucleus pulposus can cause compression of a spinal nerve at the point where it exits through the intervertebral foramen, with resulting pain and/or muscle weakness in those body regions supplied by that nerve. The most common sites for disc herniation are the L4/L5 or L5/S1 intervertebral discs, which can cause sciatica, a widespread pain that radiates from the lower back down the thigh and into the leg. Similar injuries of the C5/C6 or C6/C7 intervertebral discs, following forcible hyperflexion of the neck from a collision accident or football injury, can produce pain in the neck, shoulder, and upper limb.
Ligaments of the Vertebral Column
*This content is covered in the pre-lecture assignment and will be elaborated on in lecture.
Adjacent vertebrae are united by ligaments that run the vertebral column’s length along both its posterior and anterior aspects. These serve to resist excess forward or backward bending movements of the vertebral column, respectively.
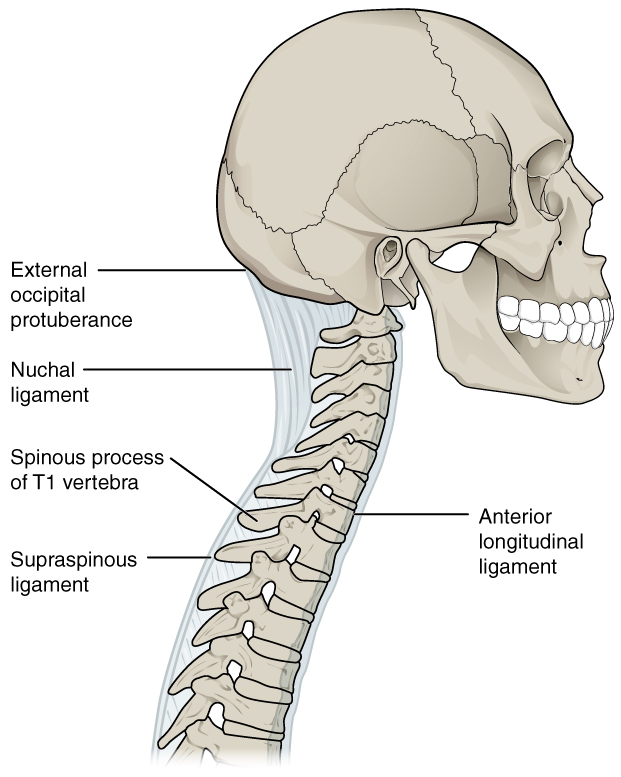
The anterior longitudinal ligament runs down the entire vertebral column’s anterior side, uniting the vertebral bodies. It serves to resist excess backward bending of the vertebral column. Protection against this movement is particularly important in the neck. Extreme posterior bending of the head and neck can stretch or tear this ligament, resulting in a painful whiplash injury. Before the mandatory installation of seat headrests, whiplash injuries were common for passengers involved in rear-end automobile collisions.
The supraspinous ligament is located on the vertebral column’s posterior side, where it interconnects the spinous processes of the thoracic and lumbar vertebrae. This strong ligament supports the vertebral column during forward bending motions. In the posterior neck, where the cervical spinous processes are short, the supraspinous ligament expands to become the nuchal ligament (nuchae = “nape” or “back of the neck”). The nuchal ligament is attached to the cervical spinous processes and extends upward and posteriorly to attach to the midline base of the skull, out to the external occipital protuberance. It supports the skull and prevents it from falling forward. This ligament is much larger and stronger in four-legged animals such as cows, where the large skull hangs off the front end of the vertebral column. You can easily feel this ligament by first extending your head backward and pressing down on the posterior midline of your neck. Then tilt your head forward, and you will fill the nuchal ligament popping out as it tightens to limit anterior bending of the head and neck.
Additional ligaments are located inside the vertebral canal, next to the spinal cord, along the length of the vertebral column. The posterior longitudinal ligament is found anterior to the spinal cord, attached to the posterior sides of the vertebral bodies. Posterior to the spinal cord is the ligamentum flavum (“yellow ligament”). This consists of a series of short, paired ligaments, each of which interconnects the lamina regions of adjacent vertebrae. The ligamentum flavum has large numbers of elastic fibers, which have a yellowish color, allowing it to stretch and then pull back. Both of these ligaments provide important support for the vertebral column when bending forward.
Articulations of the Vertebral Column
In addition to being held together by the intervertebral discs, adjacent vertebrae also articulate with each other at synovial joints formed between the superior and inferior articular processes called facet joints (zygapophysial joints). These are plane joints that provide for only limited motions between the vertebrae. The orientation of the articular processes at these joints varies in different regions of the vertebral column and serves to determine the types of motions available in each vertebral region. The cervical and lumbar regions have the greatest ranges of motion.
In the neck, the articular processes of cervical vertebrae are flattened and generally face upward or downward. This orientation provides the cervical vertebral column with extensive ranges of motion for flexion, extension, lateral flexion, and rotation. In the thoracic region, the downward projecting and overlapping spinous processes, along with the attached thoracic cage, greatly limit flexion, extension, and lateral flexion. However, the flattened and vertically positioned thoracic articular processes allow for the greatest range of rotation within the vertebral column. The lumbar region allows for considerable extension, flexion, and lateral flexion, but the orientation of the articular processes largely prohibits rotation.
The articulations formed between the skull, the atlas (C1 vertebra), and the axis (C2 vertebra) differ from the articulations in other vertebral areas and play important roles in the movement of the head. The atlanto-occipital joint is formed by the articulations between the superior articular processes of the atlas and the occipital condyles on the base of the skull. This articulation has a pronounced U-shaped curvature oriented along the anterior-posterior axis. This allows the skull to rock forward and backward, producing flexion and extension of the head. This moves the head up and down, as when shaking your head “yes.”
The atlantoaxial joint, between the atlas and axis, consists of three articulations. The paired superior articular processes of the axis articulate with the inferior articular processes of the atlas. These articulating surfaces are relatively flat and oriented horizontally. The third articulation is the pivot joint formed between the dens, which projects upward from the body of the axis, and the inner aspect of the anterior arch of the atlas. A strong ligament passes posterior to the dens to hold it in position against the anterior arch. These articulations allow the atlas to rotate on top of the axis, moving the head toward the right or left, as when shaking your head “no.”
The Thoracic Cage
*This content is covered in the pre-lecture assignment and will not be covered again in lecture.
The thoracic cage (rib cage) forms the thorax (chest) portion of the body. It consists of 12 pairs of ribs with their costal cartilages and the sternum. The ribs are anchored posteriorly to the 12 thoracic vertebrae (T1–T12). The thoracic cage protects the heart and lungs.
Sternum
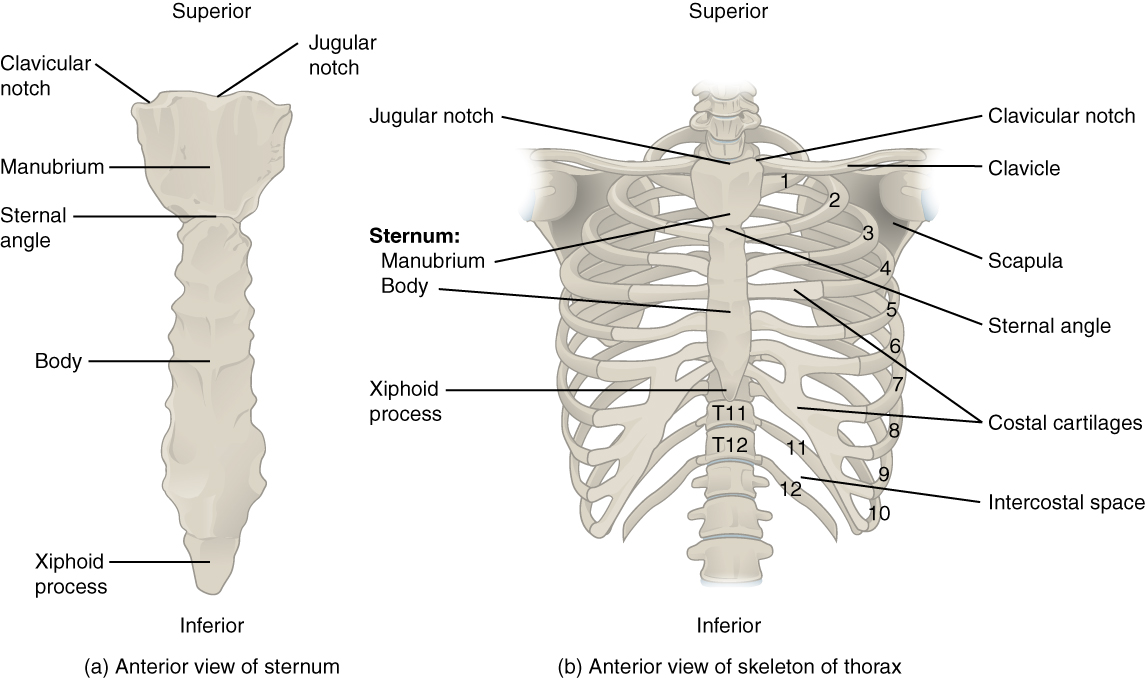
The sternum is the elongated bony structure that anchors the anterior thoracic cage. It consists of three parts: the manubrium, body, and xiphoid process. The manubrium is the wider, superior portion of the sternum. The top of the manubrium has a shallow, U-shaped border called the jugular (suprasternal) notch. This can be easily felt at the anterior base of the neck, between the medial ends of the clavicles. The clavicular notch is the shallow depression located on either side at the superior-lateral margins of the manubrium. This is the site of the sternoclavicular joint, between the sternum and clavicle. The first ribs also attach to the manubrium.
The elongated, central portion of the sternum is the body. The manubrium and body join together at the sternal angle, so-called because the junction between these two components is not flat but forms a slight bend. The second rib attaches to the sternum at the sternal angle. Since the first rib is hidden behind the clavicle, the second rib is the highest rib that can be identified by palpation. Thus, the sternal angle and second rib are important landmarks for identifying and counting the lower ribs. Ribs 3–7 attach to the sternal body.
The inferior tip of the sternum is the xiphoid process. This small structure is cartilaginous early in life but gradually becomes ossified starting during middle age.
Ribs
Each rib is a curved, flattened bone that contributes to the wall of the thorax. The ribs articulate posteriorly with the T1–T12 thoracic vertebrae, and most attach anteriorly via their costal cartilages to the sternum. There are 12 pairs of ribs. The ribs are numbered 1–12 in accordance with the thoracic vertebrae.
Parts of a Typical Rib
The posterior end of a typical rib is called the head of the rib. This region articulates primarily with the costal (demi)facet located on the body of the same numbered thoracic vertebra and, to a lesser degree, with the costal (demi)facet located on the body of the next higher vertebra. Lateral to the head is the narrowed neck of the rib. A small bump on the posterior rib surface is the tubercle of the rib, which articulates with the facet located on the transverse process of the same numbered vertebra. The remainder of the rib is the body of the rib (shaft). Just lateral to the tubercle is the angle of the rib, the point at which the rib has its greatest degree of curvature. The angles of the ribs form the most posterior extent of the thoracic cage. In the anatomical position, the angles align with the medial border of the scapula. A shallow costal groove for the passage of blood vessels and a nerve is found along the inferior margin of each rib.
Rib Classifications
The bony ribs do not extend anteriorly completely around to the sternum. Instead, each rib ends in a costal cartilage. These cartilages are made of hyaline cartilage and can extend for several inches. Most ribs are then attached, either directly or indirectly, to the sternum via their costal cartilage. The ribs are classified into three groups based on their relationship to the sternum.
Ribs 1–7 are classified as true ribs. The costal cartilage from each of these ribs attaches directly to the sternum. Ribs 8–12 are called false ribs. The costal cartilages from these ribs do not attach directly to the sternum. For ribs 8–10, the costal cartilages are attached to the cartilage of the next higher rib. Thus, the cartilage of rib 10 attaches to the cartilage of rib 9, rib 9 then attaches to rib 8, and rib 8 is attached to rib 7. The last two false ribs (11–12) are also called floating ribs. These are short ribs that do not attach to the sternum at all. Instead, their small costal cartilages terminate within the musculature of the lateral abdominal wall.
Muscles of the Abdomen
*This content will be covered in lecture.
Four pairs of abdominal muscles cover the anterior and lateral abdominal region and meet at the anterior midline. These muscles of the anterolateral abdominal wall can be divided into four groups: the external obliques, the internal obliques, the transversus abdominis, and the rectus abdominis.
| Muscles of the Abdomen | |||
|---|---|---|---|
| Movement | Target | Target motion direction | Prime mover |
| Twisting at waist; also bending to the side | Vertebral column | Rotation; lateral flexion | External obliques; internal obliques |
| Squeezing abdomen during forceful exhalations, defecation, urination, and childbirth | Abdominal cavity | Compression | Transversus abdominus |
| Sitting up | Vertebral column | Flexion | Rectus abdominis |
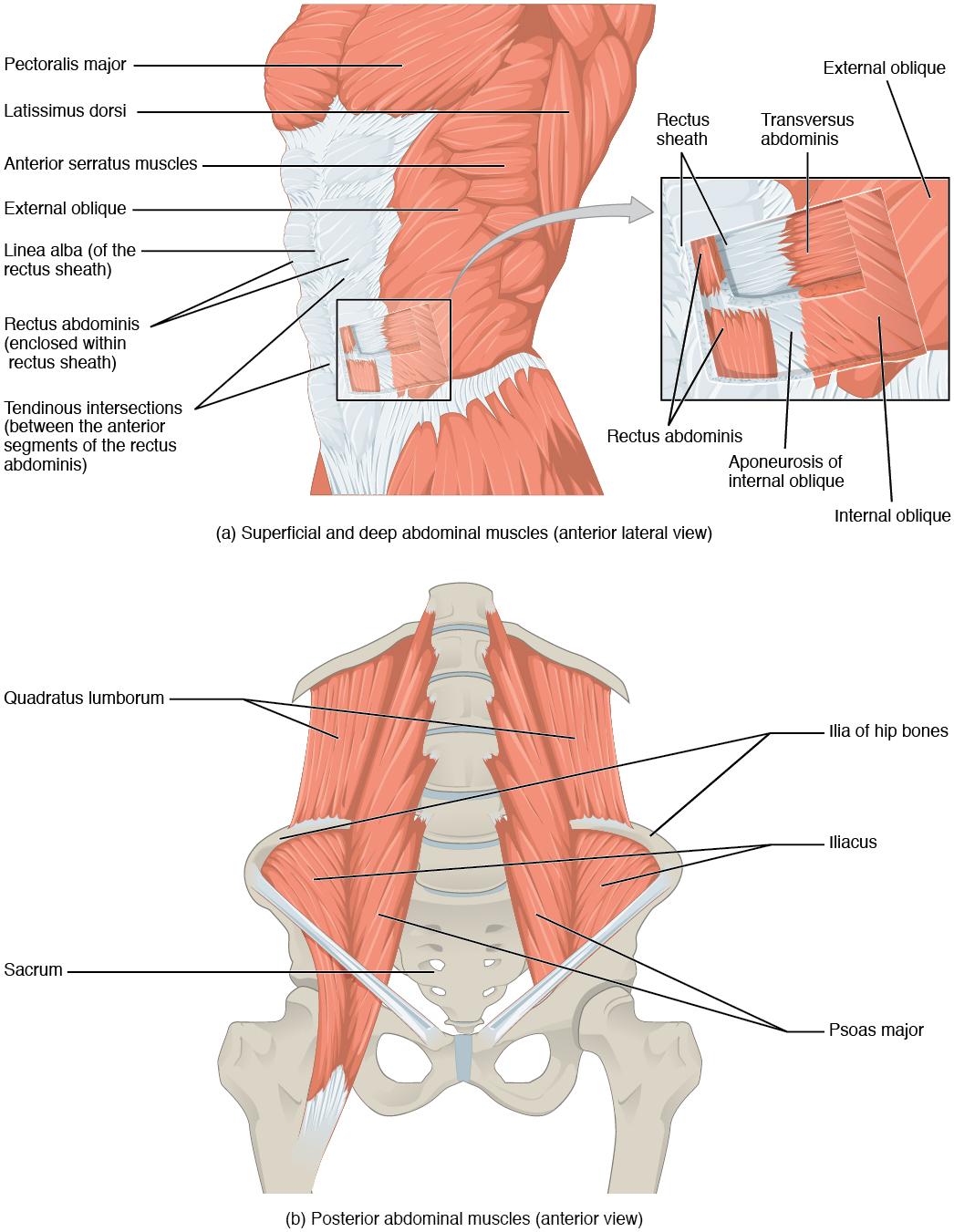
There are three flat skeletal muscles in the anterolateral wall of the abdomen. The external oblique, closest to the surface, extend inferiorly and medially, in the direction of sliding one’s four fingers into pants pockets. Perpendicular to it is the intermediate internal oblique, extending superiorly and medially, the direction the thumbs usually go when the other fingers are in the pants pocket. The deep muscle, the transversus abdominis, is arranged transversely around the abdomen, similar to the front of a belt on a pair of pants. This arrangement of three bands of muscles in different orientations allows various movements and rotations of the trunk. The three layers of muscle also help protect the internal abdominal organs in an area where there is no bone.
The linea alba is a white, fibrous band that is made of the bilateral rectus sheaths that join at the anterior midline of the body. These enclose the rectus abdominis muscles (a pair of long, linear muscles, commonly called the “sit-up” muscles) that originate at the pubic crest and symphysis and extend the length of the body’s trunk. Each muscle is segmented by three transverse bands of collagen fibers called the tendinous intersections. This results in the look of “six-pack abs,” as each segment hypertrophies on individuals who train them and have low body fat.
The posterior abdominal wall is formed by the lumbar vertebrae, parts of the ilia of the hip bones, psoas major and iliacus muscles, and quadratus lumborum muscle. This part of the core plays a key role in stabilizing the rest of the body and maintaining posture.
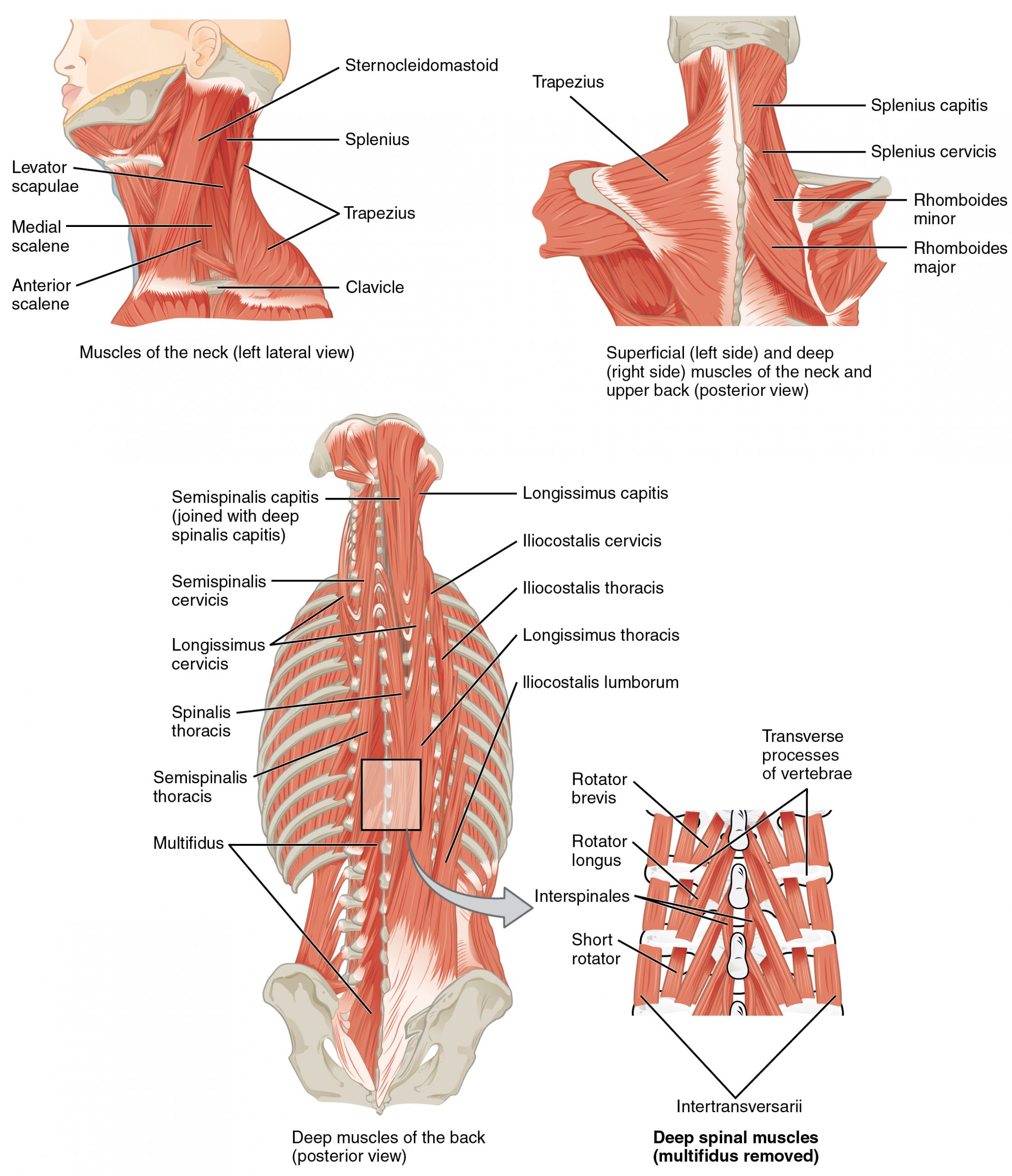
Muscles of the Back
The back muscles stabilize and move the vertebral column and are grouped according to the lengths and direction of the fascicles.
The erector spinae group forms most of the back’s muscle mass, and it is the primary extensor of the vertebral column. It controls flexion, lateral flexion, and rotation of the vertebral column and maintains the lumbar curve. The erector spinae comprises the iliocostalis (laterally placed) group, the longissimus (intermediately placed) group, and the spinalis (medially placed) group.