
Module 30: Upper Extremity II – Bones and Joints | Pectoral Girdle and Arm
Learning Objectives:
By the end of this class, students will be able to:
- List the bones of the pectoral girdle, arm, forearm, wrist, and hand.
- Establish relationships between bony landmarks and attachments of muscles/tendons or neurovascular structures in the upper extremities.
- Identify the joints and types of joints in the upper extremity and infer how muscle actions will create movement about the joint.
- Explain how the bones articulate with each other and with the axial skeleton.
- Review the innervation of muscles of the pectoral region and arm.
- Review the bones of the pectoral girdle and arm
- Relate bony landmarks of the scapula and humerus to attachment sites for muscles/tendons/ligaments or where neurovascular structures travel on or around
- List the muscles of the pectoral girdle and arm, describe their action(s), origins, insertions, innervations, and arterial supply.
- Describe how muscle actions will create movement about the scapulothoracic and glenohumeral joint
Terms to Know
|
Bones
|
Joints
Muscles
|
Bones of the upper extremity
*NOTE – All bones and bony markings will be presented in this section of the reader, but each will be reviewed as they relate to each module.
The table below highlights the bones of the upper extremity, the bony landmarks, and their associated anatomical structures.
| Bone | Bony Landmark | Associated Structures |
| Clavicle | Acromial end | Articulates with the acromion process of the scapula |
| Sternal end | Articulates with the sternum | |
| Scapula | Glenoid fossa | Articulates with the head of the humerus |
| Coracoid process | Attachment site for the coracobrachialis, short head of the biceps brachii, & pectoralis minor muscles & coracoclavicular ligament | |
| Acromion process | Articulates with the clavicle, attachment for the middle part of the deltoid | |
| Scapular spine | Separates the supraspinous and infraspinous fossa, attachment for the deltoid and trapezius muscles | |
| Medial border | Attachment for the levator scapulae, rhomboid major, rhomboid minor, & serratus anterior (anterior portion of the medial border) | |
| Lateral border | Attachment for teres minor | |
| Superior border | No attachments | |
| Inferior angle | Attachment site for the teres major muscle | |
| Superior angle | Attachment for the levator scapulae | |
| Subscapular fossa | Fossa on the anterior scapula that holds the subscapularis muscle | |
| Supraspinous fossa | Fossa on the posterior surface that holds the supraspinatus | |
| Infraspinous fossa | Fossa on the posterior surface that holds the infraspinatus | |
| Supraglenoid tubercle | Attachment for the long head of the biceps brachii | |
| Infraglenoid tubercle | Attachment for the long head of the triceps | |
| Suprascapular notch | Passageway for the suprascapular nerve | |
| Humerus | Head | Articulates with the glenoid fossa of the scapula |
| Anatomical neck | Just distal to the head of the humerus | |
| Surgical neck | Common site for fractures of the humerus | |
| Deltoid tuberosity | Attachment for the deltoid muscle | |
| Lesser tubercle | Attachment for the subscapularis muscle (and teres major) | |
| Greater tubercle | Attachment for the supraspinatus, infraspinatus, and teres minor | |
| Intertubercular sulcus (groove) | Passageway for the tendon of the long head of the biceps; attachment for the latissimus dorsi and teres major muscles | |
| Radial groove | Radial nerve travels here on its course around the posterior humerus | |
| Medial epicondyle | Attachment site for muscles of the anterior forearm (flexors and pronator teres) | |
| Lateral epicondyle | Attachment site for muscles of the posterior forearm (extensors and supinator) | |
| Lateral supracondylar ridge | Attachment site for some posterior forearm muscles | |
| Medial supracondylar ridge | Attachment site for some anterior forearm muscles | |
| Capitulum | Articulates with the head of the radius | |
| Trochlea | Articulates with the ulna | |
| Radial fossa | Space for radius during elbow flexion | |
| Coronoid fossa | Space for the coronoid process of the ulna during elbow flexion | |
| Olecranon fossa | Space for the olecranon process of the ulna during elbow extension | |
| Ulna | Trochlear notch | Articulates with the trochlea of the humerus |
| Olecranon process | Attachment for the triceps brachii | |
| Coronoid process | Attachment for ligaments of the elbow | |
| Radial notch | Distal articulation with the head of the radius | |
| Head | Articulates distally with the radius and with carpal bones | |
| Styloid process | Attachment for a ligament of the wrist | |
| Radius | Head | Articulates with the ulna and humerus |
| Radial tuberosity | Attachment for the biceps brachii tendon | |
| Styloid process | Attachment site for the brachioradialis muscle | |
| Ulnar notch | Distal articulation with the ulna | |
| Carpals | Scaphoid |
Proximal row – most lateral (most common carpal bone fractured) |
| Lunate | Proximal row | |
| Triquetrum | Proximal row | |
| Pisiform | Proximal row – most medial | |
| Trapezium | Distal row – most lateral | |
| Trapezoid | Distal row | |
| Capitate | Distal row | |
| Hamate | Distal row – most medial | |
| Metacarpals | I-V | I = metacarpal of the first ray (thumb), V = metacarpal of fifth ray (pinky) |
| Phalanges | Proximal | Digits I-V have one = 5 total |
| Middle | Digits II-V have one = 4 total | |
| Distal | Digits I-V have one = 5 total |
Bones of the Pectoral Girdle
This content will be covered in the assignment and reviewed in lecture.
The pectoral girdle consists of the clavicle and the scapula, which serve to attach the upper limb to the sternum of the axial skeleton.
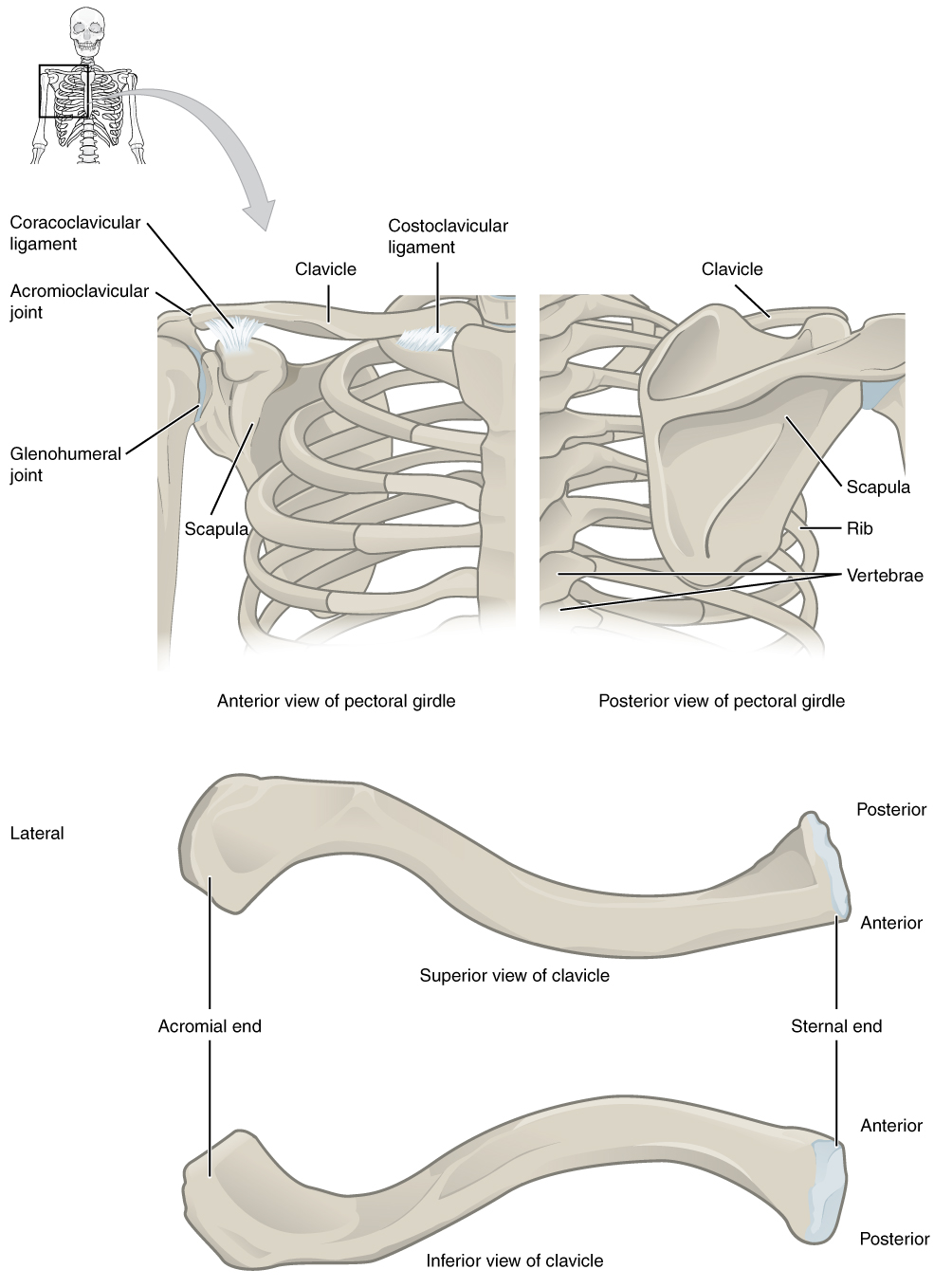
The scapula (shoulder blade) lies on the posterior aspect of the shoulder. It is supported by the clavicle, which also articulates with the humerus (arm bone) to form the shoulder joint. The scapula is a flat, triangular-shaped bone with a prominent ridge running across its posterior surface. This ridge extends out laterally, where it forms the bony tip of the shoulder and joins with the lateral end of the clavicle. By following along the clavicle, you can palpate out to the bony tip of the shoulder, and from there, you can move back across your posterior shoulder to follow the ridge of the scapula. Move your shoulder around and feel how the clavicle and scapula move together as a unit. These bones serve as important attachment sites for muscles that aid with movements of the shoulder and arm.
The right and left pectoral girdles are not joined to each other, allowing each to operate independently. Also, the clavicle of each pectoral girdle is anchored to the axial skeleton by a single, highly mobile joint. This allows for the extensive mobility of the entire pectoral girdle, which enhances movements of the shoulder and upper limb.
Clavicle
The clavicle is the only long bone that lies in a horizontal position in the body. The clavicle has several important functions. First, anchored by the muscles above, it serves as a strut that extends laterally to support the scapula. This, in turn, holds the shoulder joint superiorly and laterally from the body trunk, allowing for maximal freedom of motion for the upper limb. The clavicle also transmits forces acting on the upper limb to the sternum and axial skeleton. Finally, it protects the underlying nerves and blood vessels as they pass between the trunk of the body and the upper limb.
The clavicle has three regions: the medial end, the lateral end, and the shaft. The medial end, known as the sternal end of the clavicle, has a triangular shape and articulates with the manubrium portion of the sternum. This forms the sternoclavicular joint, which is the only bony articulation between the pectoral girdle of the upper limb and the axial skeleton. This joint allows considerable mobility, enabling the clavicle and scapula to move in upward/downward and anterior/posterior directions during shoulder movements. The lateral or acromial end of the clavicle articulates with the acromion of the scapula, the portion of the scapula that forms the bony tip of the shoulder.
Clavicle – Fun Facts? (-> you will not be assessed on this content)
The clavicle is the most commonly fractured bone in the body. Such breaks often occur because of the force exerted on the clavicle when a person falls onto their outstretched arms or when the lateral shoulder receives a strong blow. Because the sternoclavicular joint is strong and rarely dislocated, excessive force results in the breaking of the clavicle, usually between the middle and lateral portions of the bone. If the fracture is complete, the shoulder and lateral clavicle fragment will drop due to the weight of the upper limb, causing the person to support the sagging limb with their other hand. Muscles acting across the shoulder will also pull the shoulder and lateral clavicle anteriorly and medially, causing the clavicle fragments to override. The clavicle overlies many important blood vessels and nerves for the upper limb. Fortunately, due to the anterior displacement of a broken clavicle, these structures are rarely affected when the clavicle is fractured.
Scapula
The scapula is also part of the pectoral girdle and thus plays an important role in anchoring the upper limb to the body. The scapula is located on the posterior side of the shoulder and creates a functional joint, the scapulothoracic joint, with the thoracic cage. A functional joint acts as a joint, without the bony articulations, allowing for movement of the scapula on the thoracic cage. It is surrounded by muscles on both its anterior (deep) and posterior (superficial) sides and thus does not articulate with the ribs of the thoracic cage.
The scapula has several important landmarks. The three margins or borders of the scapula, named for their positions within the body, are the superior border of the scapula, the medial border of the scapula, and the lateral border of the scapula. The suprascapular notch is located lateral to the midpoint of the superior border. The corners of the triangular scapula, at either end of the medial border, are the superior angle of the scapula, located between the medial and superior borders, and the inferior angle of the scapula, located between the medial and lateral borders. The inferior angle is the most inferior portion of the scapula. It is particularly important because it serves as the attachment point for several powerful muscles involved in shoulder and upper limb movements. The remaining corner of the scapula, between the superior and lateral borders, is the location of the glenoid cavity (glenoid fossa). This shallow depression articulates with the humerus bone of the arm to form the glenohumeral joint (shoulder joint). The small bony bumps located immediately above and below the glenoid cavity are the supraglenoid tubercle and the infraglenoid tubercle. These provide attachments for muscles of the arm.
Scapula
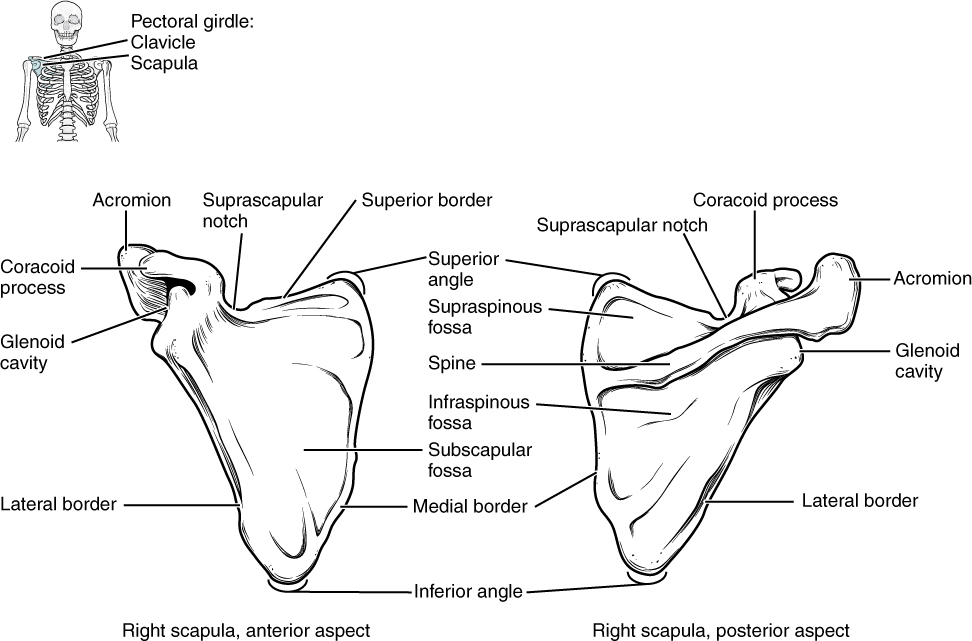
The scapula also has two prominent projections. Toward the lateral end of the superior border, between the suprascapular notch and glenoid cavity, is the hook-like coracoid process (coracoid = “shaped like a crow’s beak”). This process projects anteriorly and curves laterally. At the shoulder, the coracoid process is located inferior to the lateral end of the clavicle. It is anchored to the clavicle by a strong ligament and serves as the attachment site for muscles of the anterior chest and arm. On the posterior aspect, the spine of the scapula is a long and prominent ridge that runs across its upper portion. Extending laterally from the spine is a flattened and expanded region called the acromion or acromial process. The acromion forms the bony tip of the superior shoulder region and articulates with the lateral end of the clavicle, forming the acromioclavicular joint. Together, the clavicle, acromion, and spine of the scapula form a V-shaped bony line that provides for the attachment of neck and back muscles that act on the shoulder, as well as muscles that pass across the shoulder joint to act on the arm.
The scapula has three depressions, each of which is called a fossa (plural = fossae). Two of these are found on the posterior scapula, above and below the scapular spine. Superior to the spine is the narrow supraspinous fossa, and inferior to the spine is the broad infraspinous fossa. The anterior (deep) surface of the scapula forms the broad subscapular fossa. These fossae provide large surface areas for the attachment of muscles that cross the shoulder joint to act on the humerus.
The AC Joint – Fun Facts (-> you will not be assessed on this content)
The acromioclavicular joint transmits forces from the upper limb to the clavicle. The ligaments around this joint are relatively weak. A hard fall onto the elbow or outstretched hand can stretch or tear the acromioclavicular ligaments, resulting in a moderate injury to the joint. However, the primary support for the acromioclavicular joint comes from a very strong ligament called the coracoclavicular ligament. This connective tissue band anchors the coracoid process of the scapula to the inferior surface of the acromial end of the clavicle. It thus provides important indirect support for the acromioclavicular joint. Following a strong blow to the lateral shoulder, such as when a hockey player is driven into the boards, a complete dislocation of the acromioclavicular joint can result. In this case, the acromion is thrust under the acromial end of the clavicle, resulting in ruptures of both the acromioclavicular and coracoclavicular ligaments. The scapula then separates from the clavicle, with the weight of the upper limb pulling the shoulder downward. This dislocation injury of the acromioclavicular joint is known as a “shoulder separation” and is common in contact sports such as hockey, football, or martial arts.
Bones of The Upper Extremity
This content will be covered reviewed in this and upcoming lectures.
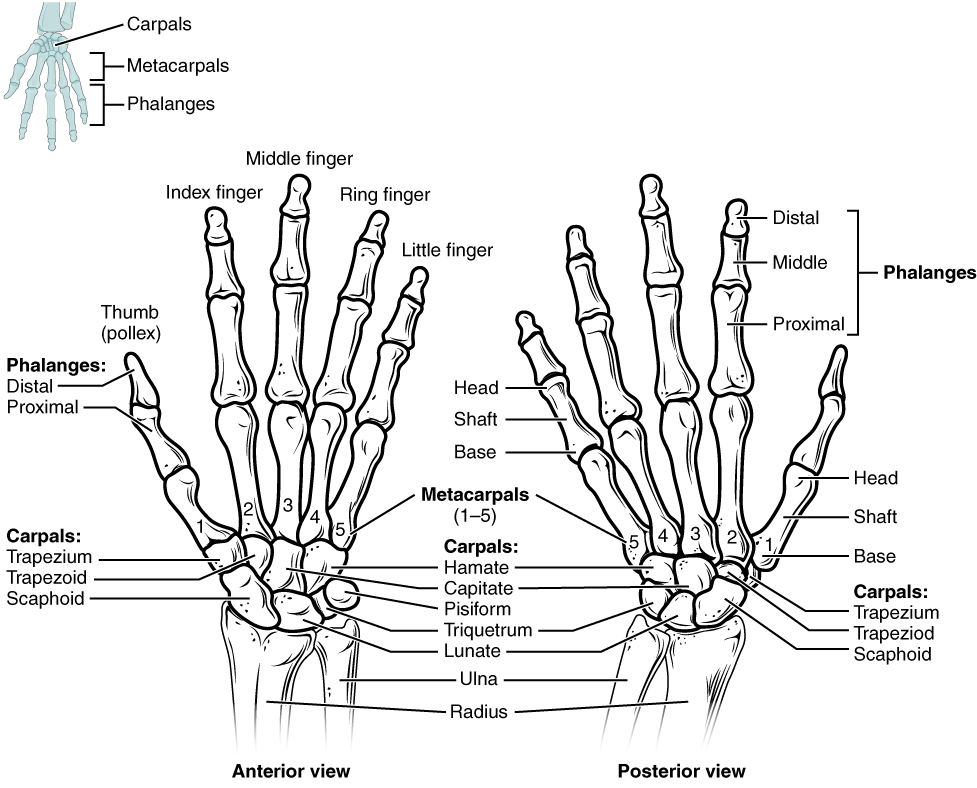
The upper limb is divided into three regions. These consist of the arm, located between the shoulder and elbow joints; the forearm, which is between the elbow and wrist joints; and the hand, which is located distal to the wrist. There are 30 bones in each upper limb. The humerus is the single bone of the upper arm, and the ulna (medially) and the radius (laterally) are the paired bones of the forearm. The base of the hand contains eight bones, each called a carpal bone, and the palm of the hand is formed by five bones, each called a metacarpal bone. The fingers and thumb contain a total of 14 bones, each of which is a phalanx bone of the hand.
Humerus
The humerus is the single bone of the upper arm region. At its proximal end is the head of the humerus. This is the large, round, smooth region that faces medially. The head articulates with the glenoid cavity of the scapula to form the glenohumeral (shoulder) joint. The margin of the smooth area of the head is the anatomical neck of the humerus. Located on the lateral side of the proximal humerus is an expanded bony area called the greater tubercle. The smaller lesser tubercle of the humerus is found on the anterior aspect of the humerus. Both the greater and lesser tubercles serve as attachment sites for muscles that act across the shoulder joint. Passing between the greater and lesser tubercles is the narrow intertubercular groove (sulcus), which is also known as the bicipital groove because it provides passage for a tendon of the biceps brachii muscle. The surgical neck is located at the base of the expanded, proximal end of the humerus, where it joins the narrow shaft of the humerus. The surgical neck is a common site of arm fractures. The deltoid tuberosity is a roughened, V-shaped region located on the lateral side in the middle of the humerus shaft. As its name indicates, it is the site of attachment for the deltoid muscle.
Humerus
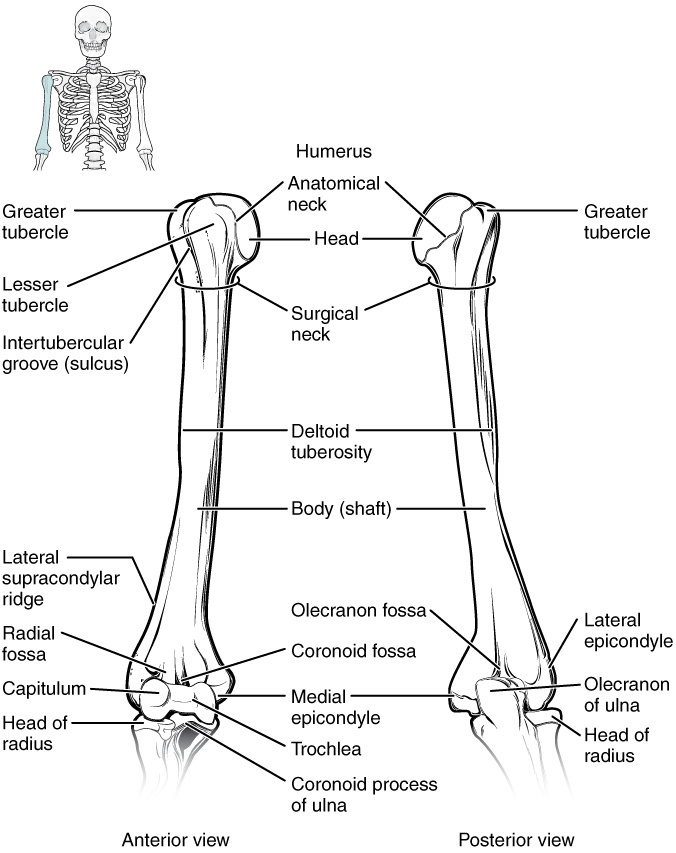
Distally, the humerus becomes flattened. The prominent bony projection on the medial side is the medial epicondyle of the humerus. The much smaller lateral epicondyle of the humerus is found on the lateral side of the distal humerus. The roughened ridge of bone above the lateral epicondyle is the lateral supracondylar ridge. These areas are attachment points for muscles that act on the forearm, wrist, and hand. The powerful grasping muscles of the anterior forearm arise from the medial epicondyle, which is larger and more robust than the lateral epicondyle that gives rise to the weaker posterior forearm muscles.
The distal end of the humerus has two articulation areas, which join the ulna and radius bones of the forearm to form the elbow joint. The more medial of these areas is the trochlea, a spindle- or pulley-shaped region (trochlea = “pulley”), articulating with the ulna bone. Immediately lateral to the trochlea is the capitulum (“small head”), a knob-like structure located on the anterior surface of the distal humerus. The capitulum articulates with the radius bone of the forearm. Just above these bony areas are two small depressions. These spaces accommodate the forearm bones when the elbow is fully bent (flexed). Superior to the trochlea is the coronoid fossa, which receives the coronoid process of the ulna, and above the capitulum is the radial fossa, which receives the head of the radius when the elbow is flexed. Similarly, the posterior humerus has the olecranon fossa, a larger depression that receives the olecranon process of the ulna when the forearm is fully extended.
Ulna
The ulna is the medial bone of the forearm. It runs parallel to the radius, which is the lateral bone of the forearm. The proximal end of the ulna resembles a crescent wrench with its large, C-shaped trochlear notch. This region articulates with the trochlea of the humerus as part of the elbow joint. The inferior margin of the trochlear notch is formed by a prominent lip of bone called the coronoid process of the ulna. Just below this on the anterior ulna is a roughened area called the ulnar tuberosity. To the lateral side and slightly inferior to the trochlear notch is a small, smooth area called the radial notch of the ulna. This area is the articulation site between the proximal radius and the ulna, forming the proximal radioulnar joint. The posterior and superior portions of the proximal ulna make up the olecranon process, which forms the bony tip of the elbow.
Ulna and Radius
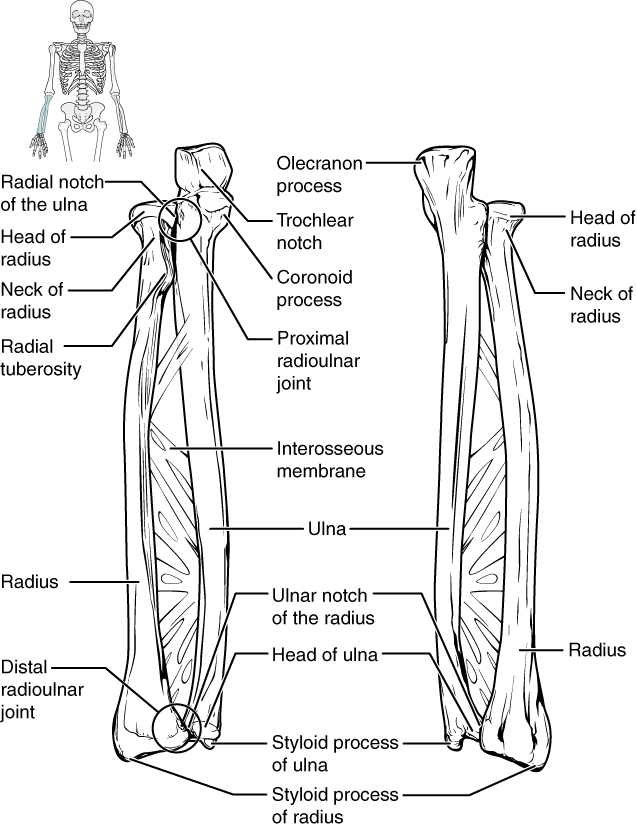
More distal is the shaft of the ulna. The lateral side of the shaft forms a ridge called the interosseous border of the ulna. This is the line of attachment for the interosseous membrane of the forearm, a sheet of dense connective tissue that unites the ulna and radius bones. The small, rounded area that forms the distal end is the head of the ulna. Projecting from the posterior side of the ulnar head is the styloid process of the ulna, a short bony projection. This serves as an attachment point for a connective tissue structure that unites the distal ends of the ulna and radius.
The Ulna – Fun Facts (-> you will not be assessed on this content)
In the anatomical position, with the elbow fully extended and the palms facing forward, the arm and forearm do not form a straight line. Instead, the forearm deviates laterally by 5–15 degrees from the line of the arm. This deviation is called the carrying angle. It allows the forearm and hand to swing freely or to carry an object without hitting the hip. The carrying angle is larger in females to accommodate their wider pelvis.
Radius
The radius runs parallel to the ulna, on the lateral (thumb) side of the forearm. The head of the radius is a disc-shaped structure that forms the proximal end. The small depression on the surface of the head articulates with the capitulum of the humerus as part of the elbow joint, whereas the smooth, outer margin of the head articulates with the radial notch of the ulna at the proximal radioulnar joint. The neck of the radius is the narrowed region immediately below the expanded head. Inferior to this point on the medial side is the radial tuberosity, an oval-shaped, bony protuberance that serves as a muscle attachment point. The shaft of the radius is slightly curved and has a small ridge along its medial side. This ridge forms the interosseous border of the radius, which, like the similar border of the ulna, is the line of attachment for the interosseous membrane that unites the two forearm bones. The distal end of the radius has a smooth surface for articulation with two carpal bones to form the radiocarpal joint or wrist joint. On the medial side of the distal radius is the ulnar notch of the radius. This shallow depression articulates with the head of the ulna, which together forms the distal radioulnar joint. The lateral end of the radius has a pointed projection called the styloid process of the radius. This provides attachment for ligaments that support the lateral side of the wrist joint. Compared to the styloid process of the ulna, the styloid process of the radius projects more distally, thereby limiting the range of movement for lateral deviations of the hand at the wrist joint.
Carpal Bones
The wrist and base of the hand are formed by a series of eight small carpal bones. The carpal bones are arranged in two rows, forming a proximal row of four carpal bones and a distal row of four carpal bones. The bones in the proximal row, running from the lateral (thumb) side to the medial side, are the scaphoid (“boat-shaped”), lunate (“moon-shaped”), triquetrum (“three-cornered”), and pisiform (“pea-shaped”) bones. The small, rounded pisiform bone articulates with the anterior surface of the triquetrum bone. The pisiform thus projects anteriorly, where it forms the bony bump that can be felt at the medial base of your hand. The distal bones (lateral to medial) are the trapezium (“table”), trapezoid (“resembles a table”), capitate (“head-shaped”), and hamate (“hooked bone”) bones. The hamate bone is characterized by a prominent bony extension on its anterior side called the hook of the hamate bone.
Bones of the Wrist and Hand
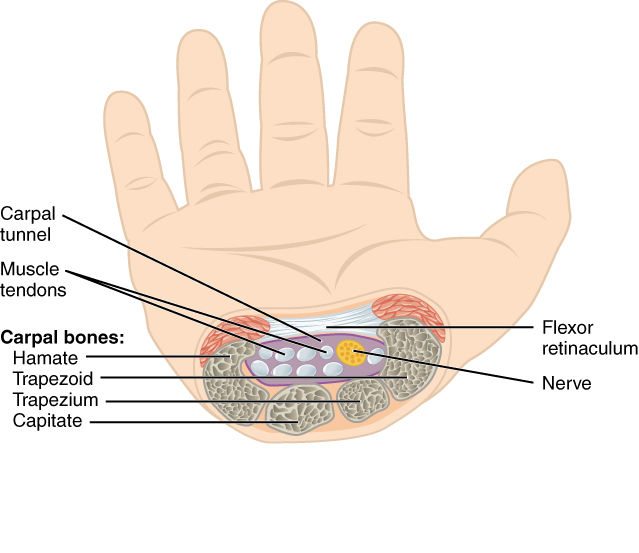
In the articulated hand, the carpal bones form a U-shaped grouping. A strong ligament called the flexor retinaculum spans the top of this U-shaped area to maintain this grouping of the carpal bones. The flexor retinaculum is attached laterally to the trapezium and scaphoid bones and medially to the hamate and pisiform bones. Together, the carpal bones and the flexor retinaculum form a passageway called the carpal tunnel, with the carpal bones forming the walls and floor and the flexor retinaculum forming the roof of this space. The tendons of nine muscles of the anterior forearm and an important nerve pass through this narrow tunnel to enter the hand. Overuse of the muscle tendons or wrist injury can produce inflammation and swelling within this space. This produces compression of the nerve, resulting in carpal tunnel syndrome, characterized by pain or numbness and muscle weakness in those areas of the hand supplied by this nerve.
Carpal Tunnel
Metacarpal Bones
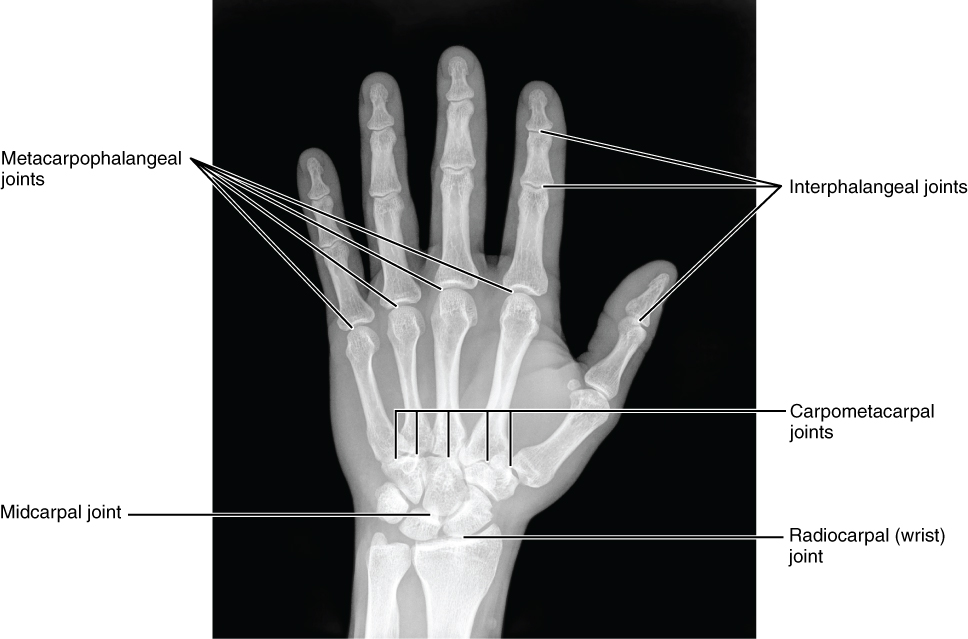
The palm contains five elongated metacarpal bones. These bones lie between the carpal bones of the wrist and the bones of the fingers and thumb. The proximal end of each metacarpal bone articulates with one of the distal carpal bones. Each of these articulations is a carpometacarpal joint. The expanded distal end of each metacarpal bone articulates at the metacarpophalangeal joint with the proximal phalanx bone of the thumb or one of the fingers. The distal end also forms the knuckles of the hand at the base of the fingers. The metacarpal bones are numbered 1–5, beginning at the thumb.
Metacarpals – Fun Facts (-> you will not be assessed on this content)
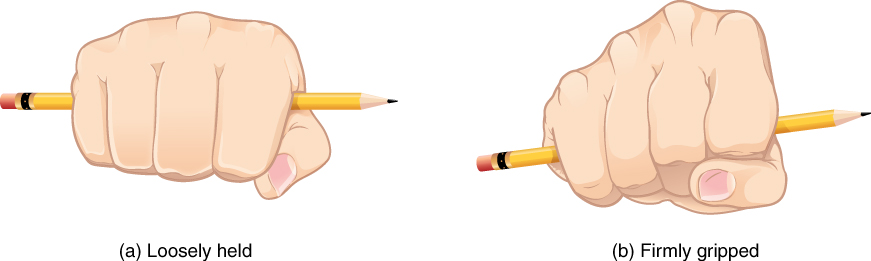
The first metacarpal bone, at the base of the thumb, is separated from the other metacarpal bones. This allows it freedom of motion independent of the other metacarpal bones, which is very important for thumb mobility. The remaining metacarpal bones are united together to form the palm. The second and third metacarpal bones are firmly anchored in place and are immobile. However, the fourth and fifth metacarpal bones have limited anterior-posterior mobility, a motion that is greater for the fifth bone. This mobility is important during power gripping with the hand. The anterior movement of these bones, particularly the fifth metacarpal bone, increases the strength of contact for the medial hand during gripping actions.
Phalanx Bones
The fingers and thumb contain 14 bones, called a phalanx bone (plural = phalanges), named after the ancient Greek phalanx (a rectangular block of soldiers). The thumb (pollex) is digit number 1 and has two phalanges, a proximal phalanx and a distal phalanx bone. Digits 2 (index finger) through 5 (pinky finger) have three phalanges, called the proximal, middle, and distal phalanx bones. An interphalangeal joint is one of the articulations between adjacent phalanges of the digits.
Upper Extremity Fractures – FYI (For Your Information -> you will not be assessed on this content)
Due to our constant use of the hands and the rest of our upper limbs, an injury to any of these areas will cause a significant loss of functional ability. Many fractures result from a hard fall onto an outstretched hand. The resulting transmission of force up the limb may result in a fracture of the humerus, radius, or scaphoid bones. These injuries are widespread in elderly people whose bones are weakened due to osteoporosis.
Falls onto the hand or elbow or direct blows to the arm can result in fractures of the humerus. Following a fall, fractures at the surgical neck, the region at which the expanded proximal end of the humerus joins with the shaft, can result in an impacted fracture, in which the distal portion of the humerus is driven into the proximal portion. Falls or blows to the arm can also produce transverse or spiral fractures of the humeral shaft.
In children, a fall onto the tip of the elbow frequently results in a distal humerus fracture. In these, the olecranon of the ulna is driven upward, resulting in a fracture across the distal humerus, above both epicondyles (supracondylar fracture), or a fracture between the epicondyles, thus separating one or both of the epicondyles from the body of the humerus (intercondylar fracture). With these injuries, the immediate concern is possible compression of the artery to the forearm due to swelling of the surrounding tissues. If compression occurs, the resulting ischemia (lack of oxygen) due to reduced blood flow can quickly produce irreparable damage to the forearm muscles. Also, four major nerves for shoulder and upper limb muscles are closely associated with different regions of the humerus, and thus, humeral fractures may also damage these nerves.
Another frequent injury following a fall onto an outstretched hand is a Colles fracture (“col-lees”) of the distal radius. This involves a complete transverse fracture across the distal radius that drives the separated distal fragment of the radius posteriorly and superiorly. This injury results in a characteristic “dinner fork” bend of the forearm just above the wrist due to the posterior displacement of the hand. This is the most frequent forearm fracture and is a common injury in persons over the age of 50, particularly in older women with osteoporosis. It also commonly occurs following a high-speed fall onto the hand during activities such as snowboarding or skating.
The most commonly fractured carpal bone is the scaphoid, often resulting from a fall onto the hand. Deep pain at the lateral wrist may yield an initial diagnosis of a wrist sprain, but a radiograph taken several weeks after the injury after tissue swelling has subsided will reveal the fracture. Due to the poor blood supply to the scaphoid bone, healing will be slow, and there is the danger of bone necrosis and subsequent degenerative joint disease of the wrist.
Joints of the Pectoral Girdle
This content will be covered in the assignment and reviewed in lecture.
| Joints of the Pectoral Girdle | |||
| Joint | Bones Articulating | Classification | Motions Available |
| Sternoclavicular (SC) Joint | Sternal end of the clavicle and the manubrium of the sternum | Saddle Joint | Elevation/Depression Protraction/Retraction Posterior Rotation |
| Acromioclavicular (AC) Joint | Acromial end of the clavicle and the acromion process of the scapula | Plane Joint | Gliding |
| Scapulothoracic Joint | NOT an articulation – scapula and thoracic cage | Functional Joint | Elevation/Depression Protraction/Retraction Superior/Inferior Rotation |
| Glenohumeral (GH, Shoulder) Joint | Glenoid fossa of the scapula and the head of the humerus | Ball-and-socket Joint | Flexion/Extension Abduction/Adduction Medial/Lateral Rotation Circumduction |
The Sternoclavicular, Acromioclavicular, and Scapulothoracic Joints
The sternoclavicular joint is a saddle joint formed by the articulation between the sternal end of the clavicle and the manubrium of the sternum. The sternoclavicular joint is the only connection between the upper extremity and thorax. There is considerable motion available in the sternoclavicular joint that coincides with the movement of the scapula on the thorax. The acromioclavicular joint is a plane joint formed by the articulation between the acromial end of the clavicle and the acromion of the scapula. The scapulothoracic joint is a functional joint, not a true articulation. Muscles on the scapula and thoracic cage prevent the bones from directly articulating, however, there is considerable movement between the scapula and thoracic cage.
The Glenohumeral (Shoulder) Joint
The shoulder joint is called the glenohumeral joint. This is a ball-and-socket joint formed by the articulation between the head of the humerus and the glenoid cavity of the scapula. This joint has the largest range of motion of any joint in the body. However, this freedom of movement is due to the lack of structural support, and thus the enhanced mobility is offset by a loss of stability.
Glenohumeral Joint
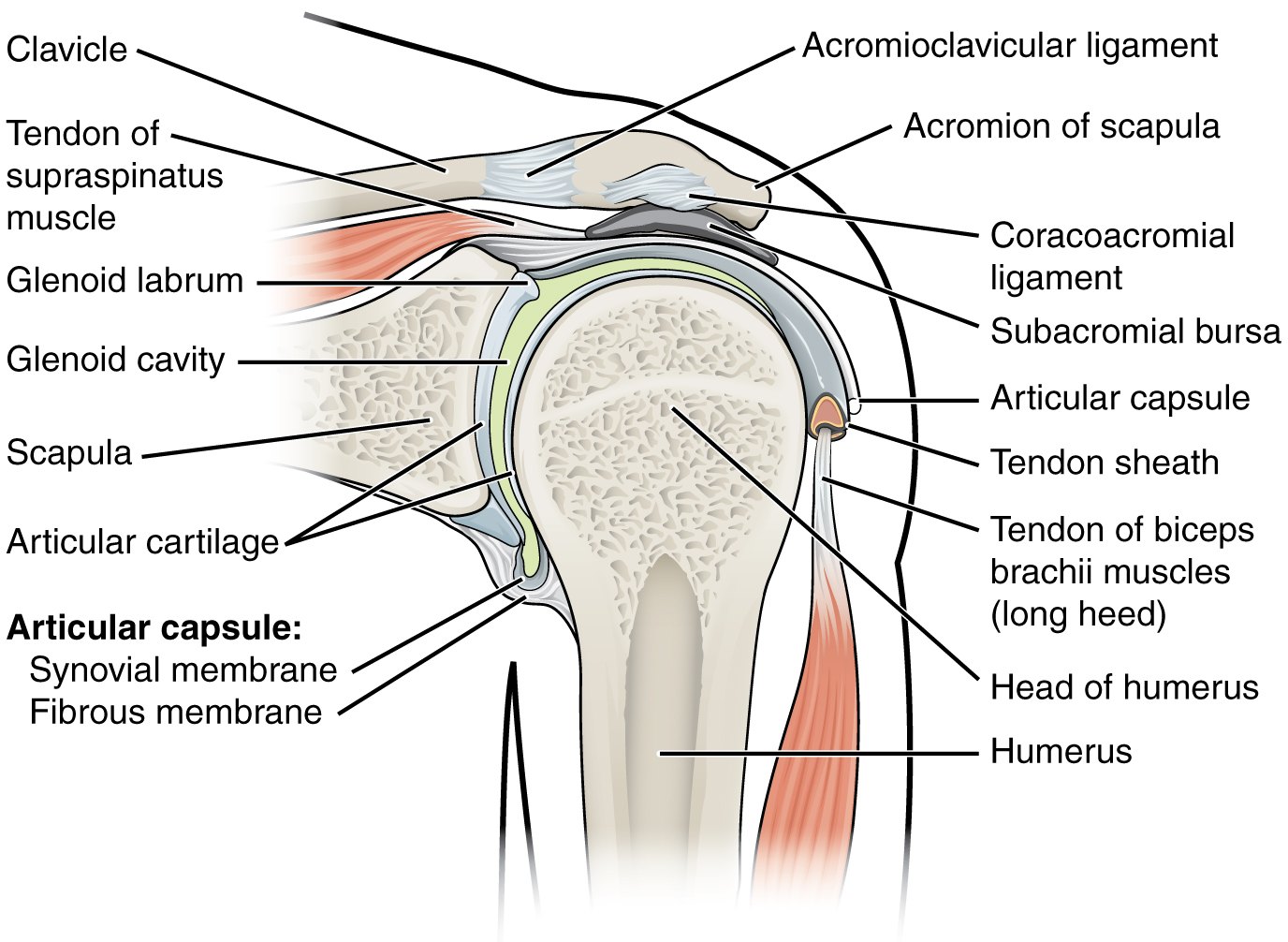
The large range of motions at the shoulder joint is provided by the articulation of the large, rounded humeral head with the small and shallow glenoid cavity, which is only about one-third of the size of the humeral head. The socket formed by the glenoid cavity is deepened slightly by a small lip of fibrocartilage called the glenoid labrum, which extends around the outer margin of the cavity. The articular capsule surrounding the glenohumeral joint is relatively thin and loose to allow for large motions of the upper limb. Some structural support for the joint is provided by thickenings of the articular capsule wall that form weak intrinsic ligaments.
The primary support for the shoulder joint is provided by muscles crossing the joint, particularly the four rotator cuff muscles. These muscles (supraspinatus, infraspinatus, teres minor, and subscapularis) arise from the scapula and attach to the greater or lesser tubercles of the humerus. As these muscles cross the shoulder joint, their tendons encircle the head of the humerus and become fused to the anterior, superior, and posterior walls of the articular capsule. The thickening of the capsule formed by the fusion of these four muscle tendons is called the rotator cuff. Two bursae, the subacromial bursa, and the subscapular bursa, help to prevent friction between the rotator cuff muscle tendons and the scapula as these tendons cross the glenohumeral joint. In addition to their individual actions of moving the upper limb, the rotator cuff muscles also serve to hold the head of the humerus in position within the glenoid cavity. By constantly adjusting their strength of contraction to resist forces acting on the shoulder, these muscles serve as “dynamic ligaments” and provide the primary structural support for the glenohumeral joint.
Injuries to the Shoulder Joint – Fun Facts (-> you will not be assessed on this content)
Injuries to the shoulder joint are common. Repetitive use of the upper limb, particularly in abduction, such as during throwing, swimming, or racquet sports, may lead to acute or chronic inflammation of the bursa or muscle tendons, a tear of the glenoid labrum, or degeneration or tears of the rotator cuff. Because the humeral head is strongly supported by muscles and ligaments around its anterior, superior, and posterior aspects, most dislocations of the humerus occur in an inferior direction. This can occur when force is applied to the humerus when the upper limb is fully abducted, as when diving to catch a baseball and landing on your hand or elbow.
Muscles of the Pectoral Girdle
This content will be covered in the assignment and reviewed in lecture.
Muscles of the shoulder and upper limb can be divided into four groups: muscles that stabilize and position the pectoral girdle, muscles that move the arm, muscles that move the forearm, and muscles that move the wrists, hands, and fingers. The pectoral girdle, or shoulder girdle, consists of the lateral ends of the clavicle and scapula, along with the proximal end of the humerus, and the muscles covering these three bones to stabilize the shoulder joint. The girdle creates a base from which the head of the humerus, in its ball-and-socket joint with the glenoid fossa of the scapula, can move the arm in multiple directions.
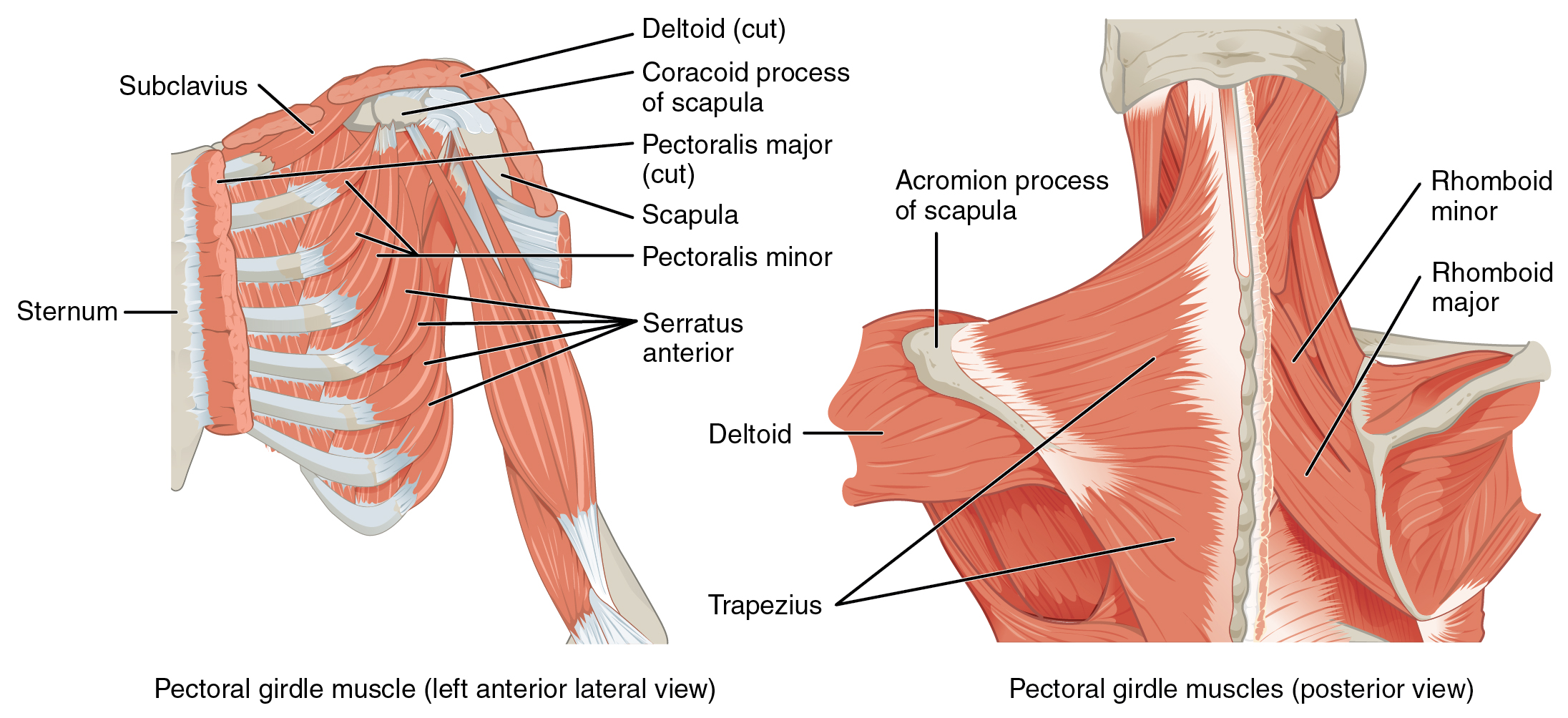
Muscles That Position the Pectoral Girdle
Muscles that position the pectoral girdle are located either on the anterior thorax or the posterior thorax. The anterior muscles include the subclavius, pectoralis minor, and serratus anterior. The posterior muscles include the trapezius, levator scapulae, rhomboid major, and rhomboid minor.
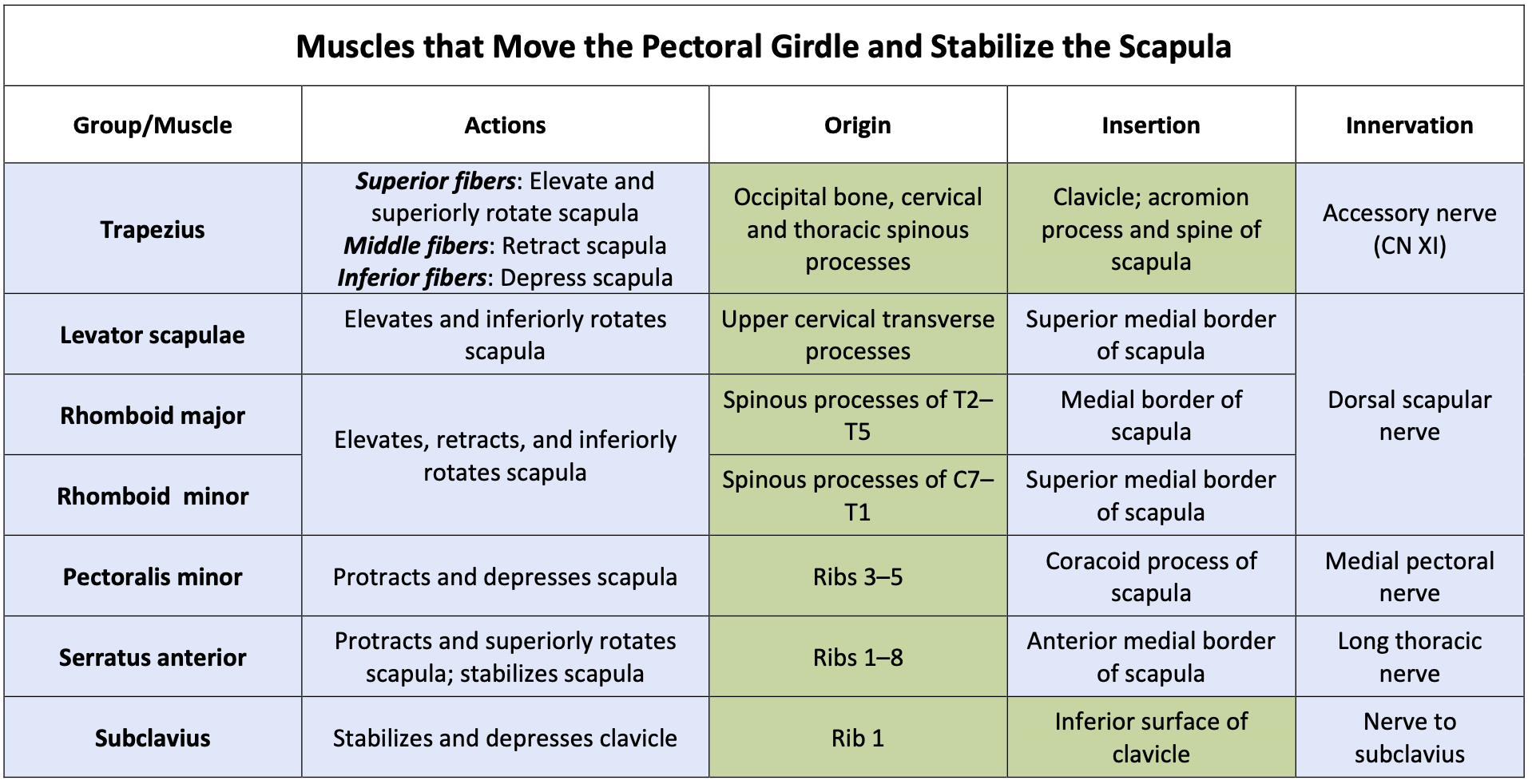
Muscles That Position the Pectoral Girdle
Use the image/table below to understand the actions, origins, insertions, and innervation of the muscles that move the pectoral girdle and stabilize the scapula.
*Note: Any box shaded in blue on the muscle chart requires you to know all the information (e.g., action, origin, insertion, and innervation) provided. Areas shaded in green require muscle identification and a general sense of the location of the origin or insertion. (e.g., knowing that the rhomboids originate on the vertebrae, as opposed to the specific numbered vertebrae).
Muscles That Move the Humerus
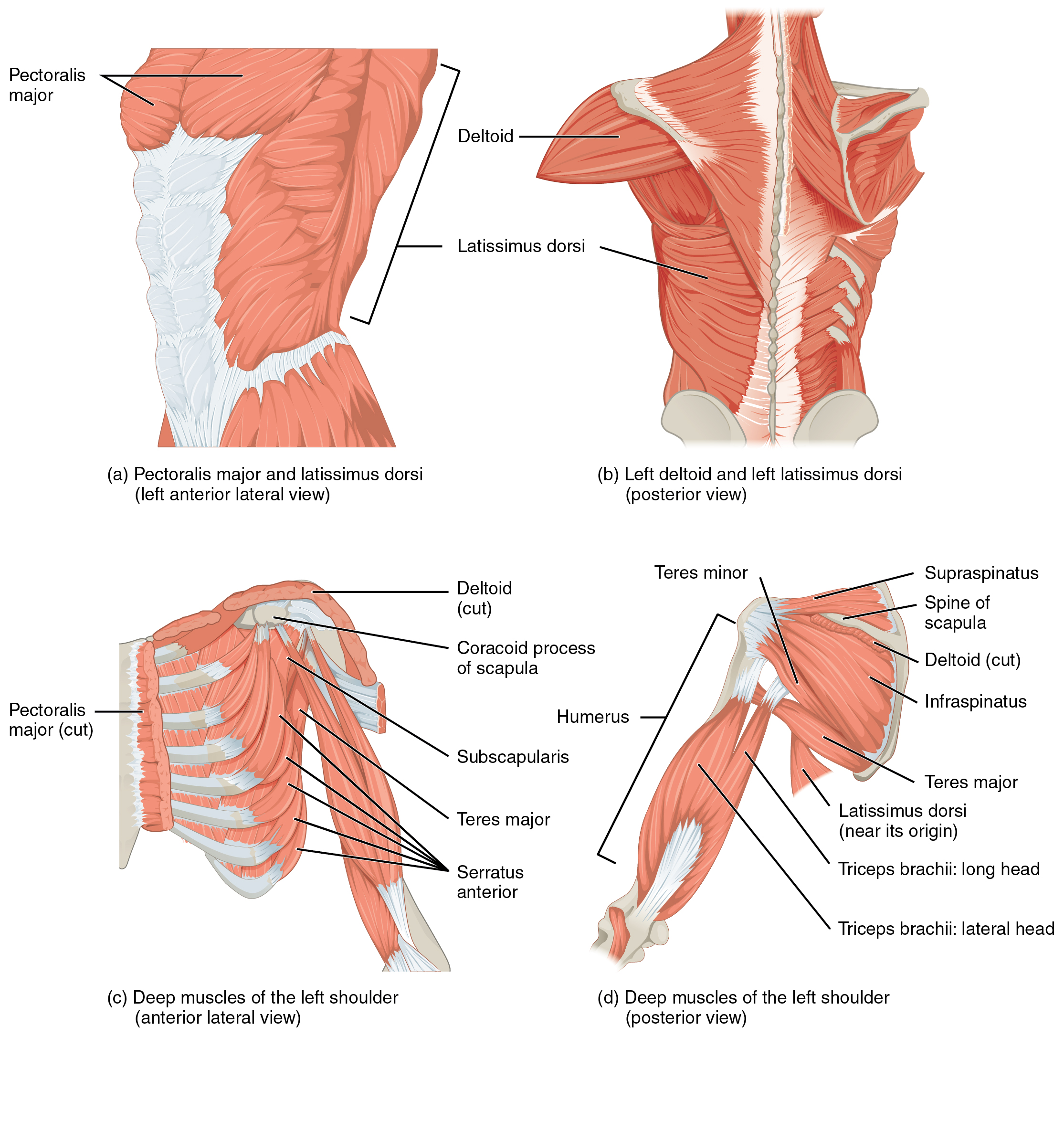
Like the muscles that position the pectoral girdle, muscles that cross the shoulder joint and move the humerus bone of the arm include both axial and scapular muscles. The two axial muscles are the pectoralis major and the latissimus dorsi. The pectoralis major is thick and fan-shaped, covering much of the superior portion of the anterior thorax. The broad, triangular latissimus dorsi is located on the inferior part of the back, where it inserts into a thick connective tissue sheath called an aponeurosis.
Muscles That Move the Humerus
Use the image/table below to understand the actions, origins, insertions, and innervation of the muscles that act on the glenohumeral joint to move the arm.
*Note: Any box shaded in blue on the muscle chart requires you to know all the information (e.g., action, origin, insertion, and innervation) provided. Areas shaded in green require muscle identification and a general sense of the location of the origin or insertion. (e.g., knowing that the rhomboids originate on the vertebrae, as opposed to the specific numbered vertebrae).
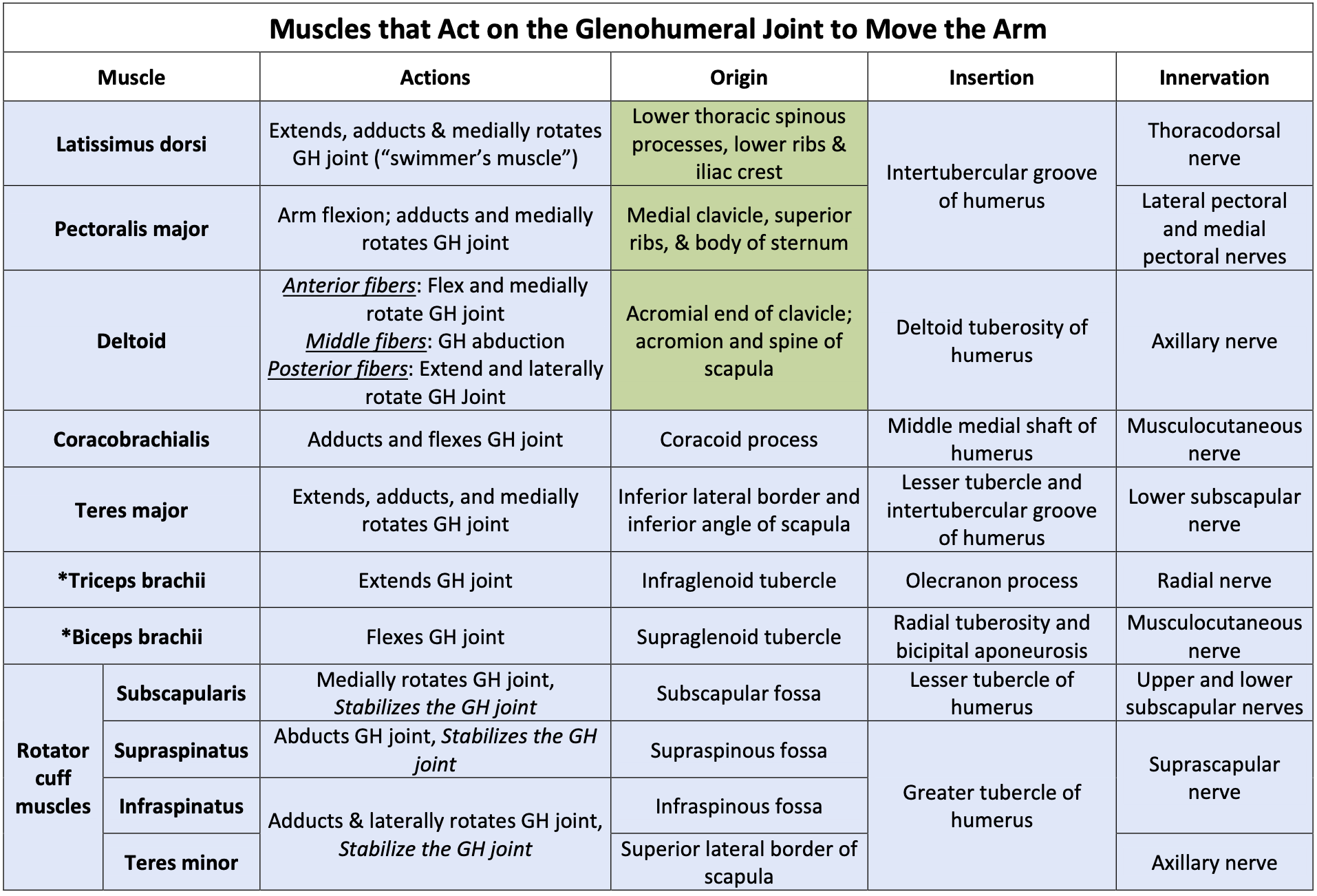
Many of the shoulder muscles originate on the scapula. The anatomical and ligamental structure of the shoulder joint and the muscles covering it allows the arm to carry out different types of movements. The deltoid, the thick muscle that creates the rounded lines of the shoulder, is the major abductor of the arm, but it also facilitates flexing and medial rotation, as well as extension and lateral rotation. The subscapularis originates on the anterior scapula and medially rotates the arm. Named for their locations, the supraspinatus (superior to the spine of the scapula) and the infraspinatus (inferior to the spine of the scapula) abduct the arm and laterally rotate the arm, respectively. The thick and flat teres major is inferior to the teres minor and extends the arm, and assists in adduction and medial rotation. The long teres minor laterally rotates and adducts the arm. Finally, the coracobrachialis flexes and adducts the arm.
The tendons of the deep subscapularis, supraspinatus, infraspinatus, and teres minor connect the scapula to the humerus, forming the rotator cuff (musculotendinous cuff), the circle of tendons around the shoulder joint. When baseball pitchers undergo shoulder surgery, it is usually on the rotator cuff, which becomes pinched and inflamed, and may tear away from the bone due to the repetitive motion of bringing the arm overhead to throw a fastpitch.
Two muscles that act on the glenohumeral joint and the elbow joint are the biceps brachii and triceps brachii. The biceps brachii flexes the shoulder joint, whereas the triceps brachii (long head only) extends the shoulder joint. Both muscles produce motions on the forearm that will be discussed in module 31.
